Ventilation in Metabolic Acidosis (Video 2)
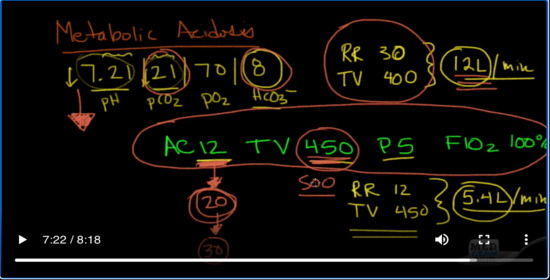
Let’s talk about another issue that I see often. Let’s talk about metabolic acidosis. So, a patient comes in with metabolic acidosis. If you remember how to deal with metabolic acidosis, you remember the Winter’s Formula. It’s just put up a blood gas here, 7.2/1/21/70/8. As you recall, this is the pH and this is the pCO2; pO2 is this third one, and then finally this is the bicarbonate.
让我们谈谈我经常看到的另一个问题。让我们谈谈代谢性酸中毒。因此,患者会出现代谢性酸中毒。如果您记得如何应对代谢性酸中毒,那就记得温特的配方。它只是在这里放了一个血气,7.2 / 1/21/70/8。您还记得,这是pH值,这是pCO2。 pO2是第三个,最后是碳酸氢盐。
So here, clearly, we’ve got a metabolic acidosis, and if you don’t remember how to do that, really quickly, if these two (pH and pCO2) are going in the same direction, then it is metabolic, and of course, they’re both down, it is a metabolic problem and that is an acidosis.
因此,在这里,很明显,我们患有新陈代谢性酸中毒,如果您不记得要怎么做,那么很快,如果这两个(pH和pCO2)朝着相同的方向发展,则它是新陈代谢,并且当然,它们都下降了,这是一个代谢问题,那就是酸中毒。
The other thing that’s a little pearl if you will, inside of a pearl, is if these two digits after the decimal point of the pH equal the digits of the pCO2 or very close to it, that usually means that it’s a pure metabolic acidosis.
这里有个小常识,那就是如果小数点后的两位数等于或接近于pCO2的位数,则通常意味着它是纯净的代谢性酸中毒。
So, let’s say you get a blood gas on a patient. And this is what it shows and here’s the bicarb, it’s pretty low, trying to compensate for that. And so, you know that this is metabolic acidosis. Your bicarb has dropped, trying to buffer whatever metabolic acidosis that was, and as a result of that, you’re trying to get rid of the carbon dioxide; it’s a Lewis acid.
因此,假设您的病人身上有血气。这就是它所显示的,这是碳酸氢盐,它很低,试图弥补这一点。因此,您知道这是代谢性酸中毒。您的碳酸氢盐下降了,试图缓冲曾经发生的任何代谢性酸中毒,结果,您试图摆脱二氧化碳。这是路易斯酸。
And in doing so, you are able to buffer your pH so that it is not so low. Okay, so you’ve got this, you’ve got the blood gas. You see the patient beforehand, and you say, you know, he’s breathing in the 30s or in the 40s, we need to intubate this patient.
这样,您就可以缓冲pH值,使其不会太低。好吧,所以您已经掌握了血气。您事先看过患者,然后说,您知道,他在30年代或40年代呼吸,我们需要给该患者插管。
Okay, maybe it’s DKA (Diabetic ketoacidosis), and the DKA has just gone on for long enough and the patient’s metabolic acidosis becomes just so severe that the patient cannot through his respirations, keep up with the work of breathing that he’s needing to do to compensate for this metabolic acidosis.
好的,也许是DKA(糖尿病酮症酸中毒); DKA进行了足够长的时间,并且患者的代谢性酸中毒变得如此严重,以至于患者无法通过呼吸来保持呼吸,因此他需要做呼吸以弥补这种代谢性酸中毒。
But for whatever reason, you take a look at this patient, and he’s breathing hard, so his respiratory rate is in the 30s. Let’s say it’s 30, and you’re able to guesstimate his tidal volume at about 400 based on how much he’s moving air. So, you do a little calculation and you come up with 30 breaths per minute times 400cc each breath, and you come up with about 12 liters of air movement per minute. So that’s his minute ventilation.
但是无论出于什么原因,您都要看一下这个病人,他呼吸困难,所以他的呼吸频率在30 s之内。假设是30,而您可以根据他移动的空气量来估算他的潮气量大约为400。因此,您进行了一些计算,得出了每分钟30次呼吸乘以每次400cc的呼吸,每分钟产生了约12升的空气运动。那就是他的一分钟通气。
So then you go and intubate the patient. And you know your protocol, or whatever your baseline is, states where you ventilate the patient, so you decide and you dial into the ventilator, AC of 12, tidal volume of 450. let’s say you put in a peep of 5 and an FIO2 of 100%. Since you’re just intubating the patient.
因此,您就可以给患者插管了。而且您知道您的方案或基准是什么,都规定了对患者进行换气的位置,因此您决定并拨入呼吸机,AC为12,潮气量为450。假设您将窥视器5和FIO2 100%。因为您只是在给病人插管。
So, to review what we talked about already, we’ve already said that this patient is going from negative pressure ventilation to positive pressure ventilation, even with a little peep of 5 on it. So, we already know that we’re going to expect our venous return to drop, our blood pressure could drop, so we need to make sure that we give plenty of fluids which were probably already doing in a patient with metabolic acidosis, whether it’s due to sepsis, or DKA because both of those involve fluid.
因此,回顾一下我们已经讨论过的内容,我们已经说过,该患者正在从负压通气转为正压通气,即使稍稍窥视5次。因此,我们已经知道我们期望静脉回流会下降,血压可能会下降,因此我们需要确保提供足够的水,这些水可能已经在患有代谢性酸中毒的患者中使用过,无论是否归因于败血症或DKA,因为两者均涉及液体。
The thing, though, that you may not realize is that this patient is actually trying to compensate for that metabolic acidosis. And by intubating, the patient usually has to give sedatives, versed, morphine, propofol, etomidate. Sometimes even paralytics are used, which means that you’ve just basically taken away their ability to compensate for this metabolic acidosis.
但是,您可能没有意识到的是,该患者实际上正在尝试弥补这种代谢性酸中毒。通过插管,患者通常必须服用镇静剂,精通吗啡,丙泊酚,依托咪酯。有时甚至使用了麻痹药,这意味着您基本上已经取消了它们补偿这种代谢性酸中毒的能力。
So instead of this being a backup rate of 12, this is going to be the respiratory rate of 12. And the patient is going to get, you know, 450 per minute. So, what you end up having here is 12 times 450. So, the respiratory rate 12, and the tidal volume is going to be 450, and you multiply those two together, and you come up with something that’s close to about, you know, 5.4 liters per minute.
因此,不是将备用频率设置为12,而是将呼吸速率设置为12。患者将获得每分钟450的速度。因此,您最终得到的结果是12乘以450。因此,呼吸频率为12,潮气量将为450,然后将这两个乘积在一起,得出的结果差不多,每分钟5.4升。
So, you can see what’s happening here, the metabolic acidosis hasn’t gone away. You’ve knocked out the patient’s drive, you’ve intubated them. Yes, but you are not meeting their metabolic demand. They’re not meeting their ventilation demand. You’ve gone from about 12 liters per minute to 5.4 liters per minute. And as a result of that, this CO2 is not going to be driven down low to compensate for this low bicarb. And what you’re going to get is the pH is going to drop even lower. And you know folks, I’ve seen it where patients have been intubated in the emergency room and they crashed afterwards just because of this.
因此,您可以看到这里发生了什么,新陈代谢性酸中毒尚未消失。您已经敲开了患者的驱动器,并已将其插管。是的,但是您不能满足他们的新陈代谢需求。他们不能满足他们的通风需求。您已经从每分钟约12升增加到每分钟5.4升。结果,该二氧化碳不会被压低以补偿这种低的碳酸氢盐。而且您将获得的pH值会下降得更低。你们知道的人,我已经看到了病人在急诊室被插管的情况,然后他们就因为这个而坠毁。
So, here’s the pearl. The point is look and see what kind of minute ventilation is occurring before you intubate. If there is compensation occurring, try to simulate that with your new vent settings, so instead of 12, you know, maybe go to 20, or even higher.
所以,这是重点知识。关键是看一下,然后再插管之前要进行什么样的分钟通气。如果发生补偿,请尝试使用新的排气孔设置模拟该补偿,因此,您知道的不是12,而是20,甚至更高。
I just saw a patient today actually who came into the emergency room with severe DKA, I mean pH of 6.8. And they intubated him, and I knew full well that this patient was going to be set on on settings close to this (20), and I wanted to make sure that that wasn’t. They actually did a good job and set the AC rate at 20. I actually set it to 30 because this patient had no COPD. She was very young, and she wasn’t breast stacking.
我今天刚看到一名患者,他进入急诊室时患有严重的DKA,我的意思是pH值为6.8。然后他们给他插了管,我非常清楚该患者将在接近此的位置上被设置(20),并且我想确保并非如此。他们实际上做得很好,将AC速率设置为20。我实际上将其设置为30,因为该患者没有COPD。她还很年轻,没有乳房堆积。
As it turned out, we just barely kept up with the metabolic acidosis. The repeat blood gas, which I recommend doing afterwards was still around 6.8, 6.9. So we gave some bicarbonate and eventually the patient’s pH improved and we’re able to pull back.
事实证明,我们几乎跟不上代谢性酸中毒。我建议之后重复做的血气仍在6.8、6.9左右。因此,我们加了碳酸氢盐,最终使患者的pH值提高了,我们可以退缩。
But that’s the other side of this. If you’re going to set these vent settings high, like to AC rate of 20 and an AC rate of 5 or TV of 500, you’re purposely hyperventilating these patients, and you’re doing so for a very good reason: you’ve got a pretty severe metabolic acidosis.
但这是另一面。如果要将这些通风口设置较高,例如AC速率为20,AC速率为5或TV为500,则有意对这些患者进行过度换气,这是有充分理由的:患有严重的代谢性酸中毒。
The thing that you’ve got to remember is as you start to fix the metabolic acidosis, you’re gonna have to re-check your vent settings. Otherwise, you can just over ventilate these patients and they’re going to have pH of 7.5 and 7.6. So, in the case of DKA, you know, the insulin drip is working, it’s starting to reduce the amount of beta-hydroxybutyrate. We’re giving bicarbonates, we are flushing the
kidney, we’re sailing to get rid of the keto acids. And so, within maybe 3, 4, 5 hours, we were able to take a pH of 6.8 and bring it up to 7.4. And we know that we needed start backing off in the ventilation, something of the body that would normally do but because now the patients on the ventilator, we have to do that for the patient.
So, second pearl is, take-home message is if you have a patient with metabolic acidosis who’s compensating above and beyond what normally would be seen,
make sure you simulate that minute ventilation when you put the patient on the ventilator, and then check it very soon afterwards to make sure that you’re keeping up with those demands. If you don’t do it, you’re going to get more acidotic and the patient is going to unravel. Okay, especially if you’ve sedated the patient for ventilation and especially if you’ve paralyzed the patient for ventilation, so just be aware of that.
Add comment