Live Webcast Replay: Key COVID-19 Clinical Updates and Lessons Learned So Far
So what we decided on covid-19 as a subject for this webcast the first person that came to mind as a speaker was Rajesh welt co-founder of medcram.com medcram.com is a leader in producing instructional videos for medical professionals and students. They provide videos to a variety of medical schools hospitals universities and their YouTube channels received over 50 million video views over the last two months medcram coronavirus pandemic updates of offered some of the most evidence.
Us-based information available most up-to-date that you could find online. So it’s with my great pleasure. I’d like to welcome Roger Schwartz to our webcast today doctor suelte is a pulmonary critical care and sleep specialist in Redlands, California. He’s a pulmonologist and sleep specialist at Beaver Medical Group where he serves on their board. He has dual academic appointments as an assistant clinical professor of medicine and physician assistants Sciences at the Loma Linda.
University School of Medicine and Allied Health Professions respectively, he is also an associate clinical professor at the University of California Riverside School of Medicine as well as medical director for the Crafton Hills College school of respiratory therapy. Finally, dr. Suelte is board certified in Internal Medicine pulmonary diseases Critical Care medicine and sleep medicine. He’s also a co-founder of medcram and speaking about medcram. We also have with us.
Today Kyle all dread Carla is a physician assistant who has practiced in both family medicine and Urgent Care. He’s director and co-founder of medcram.com and is also conference director at Wilderness medicine.com. I’d like to welcome both of you to today’s webcast. All right. Thank you so much Walter. It’s a pleasure to be here. So what we wanted to do is update on the clinical update so far and the Lessons Learned thus far with covid-19. What I wanted to do was
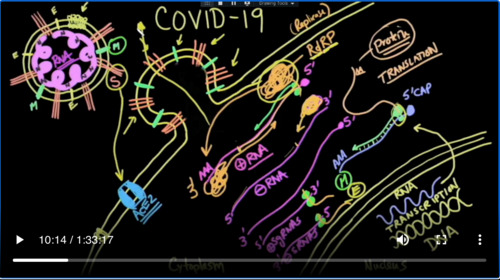
Briefly get into the path of physiology and the epidemiology and what I’ve got here is a very short seven minute video on really how does coronavirus infect human cells, you know, that’s really important because later on we’re going to be talking about how to Target these very specific areas in the pathophysiology and epidemiology of covid-19. So let’s watch this for about seven or eight minutes to give you some introduction on coronavirus, but you should be aware that the outside of this cell is
Nothing called a lipid bilayer. And actually the nucleus is a double layer of a bilayer which we don’t have to worry about but if you were to look at this very carefully there would be a hydrophilic layer on the bottom of the top and in the middle, it would be lipophilic. So it’s known as a lipid bilayer. Well, guess what? This virus also is made up of a lipid bilayer and it has a hydrophilic side on the outside and it has a
I felt like on the inside so it looks very similar. This is the reason why you can destroy viruses with detergents detergents can break that up. This virus has proteins specifically we’ll talk about the coronavirus since that’s what we are concerned about and there are proteins that are embedded in this lipid bilayer and this protein that I’m drawing here right now is called the S protein and it goes all the way through.
Through the lipid membrane. Now. There are other proteins in there. For instance. There are M proteins. There are also e proteins and they all have their specific function of structure to keep this virus intact and then what’s inside is the genome it’s a tightly packed very large RNA genome and it’s bound with n proteins. So there’s n proteins all through
Here finding the RNA molecule. So you’ve got s proteins that help bind at the end here. They are going to dock with cells you have any protein which is a membrane inside of the bilipid membrane layer. You have am protein, which is a protein also in the membrane you have n proteins which help bind it. So all of these are proteins that have to be coded by something then of course you have the RNA and that’s key here is understanding that coronavirus is an RNA.
A virus. So in this situation, we have a receptor on the surface of the human cell here, which is known as the Ace 2 receptor or a stew protein this s protein fits perfectly into that a stew and binds to it. And so when one of these comes and binds which you get at that point look something similar to this.
And you can see here that all of the viral contents comes into the cytoplasm. Well, let’s redraw this RNA molecule from the virus and you’ll start to see something very astounding.
That’s right. It’s an RNA and it has a five Prime cap. And it has a poly a tail. Just exactly as we have our messenger RNA ready for translation also notice that the cell incorporates the viral Envelope as part of its outer membrane and so as a result of that these s proteins that were there initially now become part of
Of the cellular membrane marking it potentially for cellular destruction. Meanwhile our ribosomes jump right on to this viral genome and start to March down the RNA. Now this is what’s known as a positive sense RNA and what does that mean? It means that when the ribosomes come onto this RNA and they start to go from the five Prime down to the three prime end. It’s going to
Make a protein and the protein that it makes is something called a rna-dependent RNA polymerase and so here it starts to make this protein and there it is and that’s abbreviated RNA dependent RNA polymerase otherwise known as a replicase and what this means is that this protein that is coded for by this mRNA will now take this positive stranded RNA. It’s only one.
And and it will now March from the other ends because it reads from the three prime ends and it will start to march in this direction going along the RNA and make another RNA that is complementary to the previous one here. This will be the 5 Prime end. This will be the three prime end. And of course this is going to be complementary to the original. So this will be a negative stranded RNA, but guess what this are
D RP is then going to come on to this one and start over on this side and it’s going to read down this way and the product of that is going to be the original viral genome and so you can see here that this RNA replicase is going to be making more and more rnas so that they can package these into new virulence that the cell is going to be making so it can make more virus and now the part that really blows me away when this RNA dependent RNA
Liber Ace starts to go back on again and it starts to do this. Sometimes it doesn’t reach right at the end. Sometimes it reaches from here and will only copy this part and so you’ll get a shorter RNA or it will come from this side here and we’ll get a shorter RNA. Well, when you get these shorter rnas, these are known as sub genomic rnas or SG rnas and some of them are positive and of course some of them are going to be negative because they’re complementary and
This viral RNA dependent RNA polymerase will just make more sgrna s or negative sgrna as will guess what these smaller ones also code for the smaller proteins on the virus. And so all of these rnas can be seen and read by ribosomes that the host is donating to the cause see it hijacks your cell and so these smaller proteins can be for instance and proteins which the virus needs to be.
For it and it can also be he proteins and so the virus comes into the cell and the key here that you have to understand is it gives up its RNA into the cell and it’s ready made for the ribosomes of the cell to make this protein right here called RNA dependent RNA polymerase anything that ends in an ace is an enzyme and it tells you what it does. It’s an RNA dependent which means it reads RNA and it makes
More RNA that’s what a polymerase is. It puts a little nucleotides together into a long chain with little beads and that information helps tell the ribosomes instead of making the proteins that your cell needs to make. It makes the protein that the virus wants to make and it does it in this very clever way. So the question is, how can we interrupt this? Because what happens after this is some of these ribosomes are floating around in the cytoplasm, but some of these ribosomes are actually attached to a metal.
Brain, which is contiguous with this outer membrane. And so they can insert all of those proteins just like they want and then the reverse of what happened here at the beginning occurs where these things but off and little viruses get packaged and they go off that’s how one VY run is able to go into one human being and millions and millions of viruses come out. It’s because it hijacks the molecular biology of the cells and it happens to be that these
case two receptors are generally speaking in the lower portion of your respiratory tract with all of these cellular outer membranes with all of these foreign proteins, you know, the immune system is going to start attacking these cells and that’s what happens with these lower respiratory cells, they become inflamed they leak fluid and that’s what causes the pneumonia and the respiratory failure.
So you can see very clearly that it’s an involved process and there’s many points along that way that the virus can be interrupted and that’s what we’re going to be talking about in the latter partion of today’s presentation is what is the treatment mechanisms? So the other thing that we have found very interesting is that the H2 receptor is not the only receptor that the virus attacks. It also attacks the CD 147 in the T lymphocytes as well and almost
A formerly in the patients that I take care of. They almost always have very low lymphocyte counts, which is a concerning thing because this is part of the immune system and helps the mountain response against covid-19, but the other thing that’s interesting and you may not know is that not only is Ace to the receptor for SARS Cub to and being in the lungs. It’s also found extensively through the endothelium and that’s important because as you can see here at the bottom Angiotensin,
And converting enzyme confers endothelial protection and attenuates atherosclerosis. Not only atherosclerosis but also oxidative stress Etc. And so we don’t have to go through this in detail, but many of you know that Angiotensin the renin-angiotensin system is implicated with this. We know that Angiotensin goes to Angiotensin 1 through renin and that goes to Angiotensin II and that we’re going to talk about Angiotensin II later on so keep that in mind remember that Ace.
Block Angiotensin one to go into Angiotensin II, but what you may not know is that Angiotensin II which is a vasoconstrictor, very potent. Vasoconstrictor is metabolized by a stew. Yes ace to the very same Target of stars Cove to and it metabolizes Angiotensin II which is a potent basil constrictor to Angiotensin 1 7 which is a which is a vasodilator now in situations where a stew is not able to do that and
Attention to levels increased significantly and then they are metabolized not by a stew. But the receptor for Angiotensin II is the Angiotensin receptor and this causes as you can see here the opposite vasoconstriction a RDS fluid leakage and you can see that what we’re seeing in covid-19 is very reminiscent of this pathway here of the Angiotensin II going to a stew but a stew not being able to metabolize.
Because the virus is taking a stew out of commission. And then the Angiotensin receptor is binding with Angiotensin II and causing vasoconstriction. So let’s talk a little bit about the course of the disease. No very early on in Wuhan we were getting information about how this disease when I like to call it phase one two, and three phase one being prior to infection phase two is during the incubation period And while the symptoms are building and then finally in Phase 3 when they’re
admitted to the hospital and many times. This is a very downward course Very quickly and we’ve seen that in the hospital. Let’s talk about hospitalization. There was a recent article that was published in Jama in looking at from March 1st to April 4th, and they looked at people and being admitted in the New York City area a hundred percent of these people being admitted 60 percent male 40% female. So we do see a male predilection to this interestingly only 30% of them had a fever 31% fever.
Percent of them have to go to the Intensive Care Unit in the Intensive Care Unit the median age. There was 68 years of age 66 percent of them were male and 12% of them needed mechanical ventilation overall as you can see what is very concerning though is of those people admitted to the hospital 21 percent of them had died basically had a 21 percent mortality those going to the intensive care or needing mechanical ventilation 88% of
Of them, you can see that there’s a very very high correlation with those people needing ventilation and those dying which should not surprise us.
If we look at those people by age, if greater than 65 years of age on a ventilator mortality was 97 percent. That’s extremely high percentage. All right, let’s look at the other side of it not those that are admitted to the hospital. But those that are out in the community Phase 2, we would like to call it recent studies that show at least in Southern California out of USC that doing 863 random tests showed that four point one of them 4.1%
percent of those that they tested were infected based on the fact that they had antibodies and this correlated with anywhere between 22 and 55 times higher the number that they thought they had based on confirmed tests. And so what we’re really seeing here is that we’re seeing a small tip of the iceberg in terms of people who have symptoms and then maybe about twenty percent of those are needing to go to the hospital of those 22 percent of those have a mortality rate and then of those needing mechanical
An 88% die. So let’s talk a little bit about the course of covid-19. As we were mentioning again population infection face to are those people that are symptomatic either at home or at needing to go to the hospital and I say here 80% of those have symptoms, but don’t need to go to the hospital 20% of those do need to go to the hospital. They have shortness of breath will talk about the criteria for hospitalization. And then you enter phase 3, and this is what we’re doing.
Anything we possibly can to prevent these people from dying including putting them on ventilators to support their breathing. But let’s talk about the 80% 80% of those don’t need to go to the hospital. And the reason for that is probably because of their immune system as you can see the immune system is very complicated. There’s an innate and adaptive immune system the cells that are particularly important. We’re finding out here are the natural killer cells and the monocytes for that innate immune system coverage.
And that’s important because there’s been a number of papers that have come out out of centers of excellence in Thailand that have looked at SARS cup of two in relation to the previous coronavirus has the previous contrivances being merged to back in 2012 and the original SARS back in 2002. And so they looked at those viruses and they made predictions about what they would see here with covid-19. And a lot of those predictions have come true. So let’s look real quickly and see what the major points were out of this major.
A review paper number one, they found that there was increased neutrophils and decrease lymphocytes that’s going to be important as we talk later on because neutrophils give a lot of oxidative. Burst. We’re going to find out that oxidation is the Real Enemy here with covid-19 nadph oxidase is the enzyme in neutrophils which causes oxygen to be turned into Super oxide and that actually is how neutrophils kill what they ingest. But in addition to that we saw decreased lymphocytes lymphocytes are very important in terms of the
Immune response and we saw that when there was increased neutrophils and decreased lymphocytes that increased mortality. We know that the innate immune system is the target of SARS and MERS and that it actually can hamper that and that’s why we may be seeing patients coming to the hospital needing help only 30% of them are needing or having a fever. There may be uncontrolled viral replication. We see that there is a reduction in the Adaptive immune system as well T cells
Is there is a suppressed immune response? We’re finding that out very clearly that some of the proteins in coronavirus are actually suppressing the immune system. And that’s what Ivermectin is. Hopefully trying to be able to do we also saw that there are antibodies that are being made and those antibodies have been shown to prevent reinfection in some patients. So I think it sums it up on this article at the very bottom. It says these facts strongly indicate that the innate immune response.
Response is a critical factor for disease outcome. And that kind of leads us to what a lot of people have been talking about the BCG vaccine the BCG vaccine stimulates the Adaptive immune response because it’s a vaccine you’re looking for an antibody response against tuberculosis. But what they found is that there is a spill over when the when the Adaptive immune response is activated. There’s an innate immune response, which also is activated as well and that of course is very important.
Against the coronavirus so you can see here that this adaptive immune response like natural killer cells or the Adaptive immune response when it is activated. There’s a spill over and the innate immune system is also activated. This is important because what they’re noticing with people who have the BCG vaccine in countries, there’s an improved response. It seems maybe an association but there’s definitely improve response. If you look at this map here, you’ll see that those in Orange.
Are countries that have never given the BCG vaccine countries like Canada like the United States notably Italy, although countries that are in yellow have have generally been giving the BCG vaccine and you can see that there is a quite a lot of countries in that color. The purple countries are countries that used to give the BCG vaccine but they’re not giving them any more there was a study that was done looking at the mortality rates and the incidence in these countries, and this was published by
A doctor a Sheikh Ahmad at MD Anderson in Houston, Texas, and he says while we expected to see a protective effect of BCG the magnitude of the difference almost tenfold and incidents and mortality between the countries without a BCG vaccination program was pleasantly surprising so 10-fold difference. The question is is this an association or is this causation? Well, they’re looking at this now but clearly the innate immune system is very important in the covid-19.
So let’s briefly take a pause here. We’ve talked about the app. We’ve talked about the pathophysiology. We’ve talked about the epidemiology. We’ve talked about immunity. We see here that the death rates in those the people that have been admitted to the hospital and those that are not admitted to the hospital. We do see that immunity may play a large factor in determining who survives so I want to unpack this and what we want to do next is I want to introduce the other co-founder.
Our of medcram.com Kyle all red who’s going to give us some questions? I’d like to take some questions based on the presentation so far. We’re not done yet. We’re going to go into diagnosis and treatment. But Kyle, maybe you can join us. Okay. Ryder can hear me? All right. Yes, here we go. The first questions is Peter from Melbourne. Florida wants to know if covid-19 is causing a large increase in our OS and oxidative stress. Does that imply that there is damage?
Being done to the nuclear DNA and the virus is carcinogenic. Yeah, that’s a that’s an interesting question. There’s many many diseases that we know increase reactive oxygen species like cardiovascular disease and things of that nature. I don’t know if we know about any cancers that are associated with that. However, we do have evidence that certain dietary things can cause cardiovascular disease and also are associated with Cancers but at this point
And of course it’s way too early to tell and of course reactive oxygen species is a wide spectrum. There can be a small amount and there can be a large amount. So I think at this time we don’t really know. Okay. Next question is from Sharon from Newmarket, Alabama previous comorbidity concerns with NSAIDs in SARS Cub to our their updated therapeutic prophylaxis risk-benefit considerations related.
Latest thrombosis research and per dr. Schultz Haitian observations of D-dimer levels. The first part of that question comes that nonsteroidals. I heard you say, yep nice rolls. So nonsteroidals are tricky because nonsteroidals, we know decreased platelet adhesion and they also are a bit of an anticoagulant so you can bleed more but we also know that there are certain NSAIDs that have a direct antiviral effect specifically on influenza.
Ah, and even the Stars Stars One virus the original SARS virus. The problem is though is that these NSAIDs can also negate the body’s febrile response, which is also been shown to be beneficial. So it’s really a mixed bag at this point. I know there was some press on this because the French Health Minister initially had said that there were some negative associations with patients who had come in
And sets but they’ve later retracted that and the who has as well. We really don’t have any very good studies at this point and I haven’t seen any kind of patterns in my practice. What we’ve done in our hospital is if we are going to treat a fever will do so with Tylenol rather than NSAIDs, but I can also tell you there that we become more conservative with our use of Tylenol, especially given the fact that we know that a fever can be beneficial and also because a lot of our patients have elevated liver enzymes as part of this process.
process
Excellent. Yeah, brother question, dr. Fault or yeah, we’ll take one more and then we’ll move. Okay. So this is from a paramedic this from Ken and she has a question about whether CPAP or BiPAP would be suitable treatment for these patients if they are conscious. Yeah. So if they’re conscious that’s always that’s exactly the point is you want to make sure you have mental cognizance before you put these on because if they can’t protect your Airway they can have a lot of problems. So I guess the only reason why I would say you could use
CPAP or BiPAP at home theoretically is to is to avoid hospitalization. But I think at that point if you are needing to use BiPAP or CPAP, that’s the point that you need to go to the hospital. If you have shortness of breath and you’re having a difficult time breathing, it would be better for you to be monitored and seen at the hospital and getting BiPAP and CPAP then trying to do this at home. Excellent. Well, I think you can go ahead and move on and we’ll take some more questions after your next that good. So this next segment is pretty short. It’s talking about
About diagnosis and specifically what we’re going to talk about here is the two basic tests for the diagnosis is the PCR and the and the antibody test and we’re going to watch A Brief video on those descriptions. I wanted to talk a little bit about testing. And again, I want to review there’s different types of testing that’s going on up to this point. We’ve looked at reverse transcriptase PCR and here we’re looking at the RNA of the virus itself. This is usually done by a nasal swab.
And if it’s positive it tells you that you are infected and if it goes from positive to negative generally speaking what you’re trying to find out is whether or not you’re still infective. Now. This is very different than antibody testing. So with antibodies you have a antigen presenting cell that has eaten and infected cell and is presenting a portion of the virus on its surface that connects up with a T-cell and once that connection is made.
There are cytokines which induce that T Cell to do a number of things number one the first possibility our memory cells. Number two are cytotoxic T cells and number three are B cells that turn into plasma cells and they create things called antibodies and these antibodies go out and attack the virus. So this is different. We’re not looking for RNA of the virus. We are looking for proteins or specifically
Antibodies, this is not done with the nasal swab but it’s done with the finger prick and what this tells you is whether or not you have IGG or IGM.
IGM and IGG usually come up maybe around 6 to 7 Days generally speaking after the beginning of an infection and they both sort of come up but the IGM will go away and the IGG will be the only one that remains usually and so IGM is usually seen in a cute and IGG is chronic. One of the things you should understand is just because you have the presence of antibodies. It doesn’t mean that you would be negative on the infective state. So it’s possible.
To be both positive on the reverse transcriptase PCR and also be positive on the antibody testing and that would simply mean that your body has made antibodies against the virus, but you still have the virus and you’re still infective.
Okay. So those are the two basic types of testing. The other thing that we’re looking at in terms of that in the hospital is a lot of these biomarkers. So CR key ferritin D-dimer LDH CPK and and lymphocytes if we have a question about somebody who’s coming into the hospital and we haven’t gotten the test back these often tell us whether or not this patient is a covid-19 patient or not because we can simply tell by the
Are 10 the D-dimer the LDH if these things are very high. There’s very little else that these patients could have that would do this. And so I found these to be very very helpful. It doesn’t mean if it’s negative that they don’t have it. But it’s another piece of information that you can have before you get the final covid test back also helps in terms of whether or not you might think the patient may have a false negative test if this patient is on the ventilator with super high CRPS ferritin D-dimer and they have infiltrates and their test comes back negative that might
Be one that you might want to re-check again course, this is what the CT would look like point though. Is that whereas in China? They did a lot of CT scans to make diagnosis because that was the fastest way for them to do it here in the United States the turnaround time in terms of what they have to do to clean the machine clean the room before the next patient comes in is prohibitory to doing a lot of CT scanning. So make sure that you do CT scanning on a on a very important basis to make sure that
It would change your management. So we’ll stop there in terms of diagnosis. I know sometimes there’s a lot of questions on that Kyle. Let’s let’s see if there’s any questions on the diagnosis.
So not necessarily specific to the diagnosis, but we have a viewer from Pakistan and wants to know how covid-19 is related to stroke and thrombosis. I know you talked a lot about that in this presentation and other videos on our site, but could you sum that up with a cliff notes version of that? Excellent question, so we don’t know exactly how it’s happening. But we’re definitely seeing an association. I mean 30 40 year olds in New York are presenting to the hospital with Strokes.
And no other symptoms and then they turn out to be covid positive is that an association? It’s hard to say for sure because there’s so many people now that have covid-19 and there’s a lot of people that have strokes but you really don’t see that in 30 and 40 year olds generally speaking. One of the theories is that this being an endothelial cell disease and because of the fact that there’s H2 receptors on the endothelial cells what could happen is inflammation?
Ation of those endothelial cells will cause a release of coagulation factors. We’re going to talk about that coming up. But basically you we will show you that there are releases of endothelial factor 8 von Willebrand’s factor and these are going to make the blood hypercoagulable and certainly that’s it’s not a stretch to see how that might cause stroke, but we’ll talk more about that in the and then actually coming up here very shortly. Okay got another
Ted’s question for you. This is from Darlin before covid-19 became prevalent in the u.s. French prime minister recommended not using NSAIDs for fever. Dr. Pol. Can you address the use of aspirin and other NSAIDs as anti platelets now that thrombosis issues of covid-19 are evident. Yeah. So that’s a very important thing. We just don’t know there’s two aspects do to this there’s coagulation and then there is platelet adhesion and the studies seem
to indicate that there’s high levels of factor 8 of Von Willebrand factor. This does play into the platelet because the platelet does use these things one of the things that you can use against von Willebrand’s factors are the the 3/8 to be the to P3 a Inhibitors basically, so we don’t know we just don’t know I would say at this point if somebody has to be on Aspirin because they have a stent specifically a drug-eluting stent.
They should be staying on their aspirin at this point because the covid-19 interaction with Aspirin is a big black box. We don’t really know to what degree it’s affected. We do know very clearly that there is a risk if people need to be on aspirin for specific reasons, if they stop them there is also a very large risk of thrombosis if they stop aspirin and or Plavix in those situations the same thing goes for people with Strokes.
So certainly at this point, I would say if you’re on aspirin and Plavix from your doctor, you should stay on it. If you’re a physician prescribing it and there’s a clear indication from what we know on studies that involve aspirin Plavix. You should continue to prescribe those until we find out exactly what the risks and benefits are from covid-19 because we simply don’t know and by the way, that’s the same answer that I would give for ACE inhibitors and a Arby’s we haven’t had a question on that yet, but I’m sure we will if
You’ve been prescribed the medication that may have an effect or not with covid-19. Then you just you just need to continue to do that until we find out more information because we just don’t know at this point.
Okay, let’s do one more question here. And this is from a viewer and Colorado are people with underlying conditions including age as likely to be asymptomatic carriers as compared to the general population.
Yeah, you know we haven’t really done those studies yet. It seems as though a lot of young people are the asymptomatic carriers. It seems as though that’s the case. It could also be very well the case in the elderly as well. We just don’t know it’s certainly clear that people become more symptomatic as they get older the certainly the mortality is that way but we would have to do just to find that out is to is to test people extensively and then review their
Trees and then be able to see if they have antibodies. I’m not aware of any tests that have that have looked at that specifically as yet so we would have to hold off on that. Okay. I think we can go ahead and proceed with the presentation. We’ll get to some more questions soon. Great. So this is the bulk of it. This is what everyone wants to know is the management. Okay. So let’s talk about management and I’ll just say I’ll let you know where what the official responses are with official recommendations and I’ll let you know where my personal opinions May differ on some of these things or more.
Maybe go along with what they say, but maybe a little bit different based on some evidence the labs that I think you ought to have on these patients are the CBC the CMP the CPK ferritin the PT PTT and the D-dimer with a number of these other labs like LDH troponin ECG Hepatitis, B and C and HIV. These are important in distinguishing what these patients have four other patients that might be coming in. I think a chest x-ray.
Very important, I would hold off on doing CT scans unless it’s absolutely necessary because of the turnaround time that we mentioned echocardiography is also very important, especially since the cardiovascular system is involved in this and then blood cultures are not necessarily routinely needed to be done. But if there is Need for blood cultures, then then we should do that as well when I say a need for a blood culture I’m talking about if there’s obvious a fever or new fever or there is
Rikers or chills? What about antibiotics antibiotics do not necessarily have to be prescribed. There’s not routine. If you see a super infection, then go ahead and treat all those super infection is not very common in covid-19 getting a Gram stain culture sensitivity is important and if you notice that there is an infection in using the regular idsa guidelines are important. So if it’s a community acquired consider using a third-generation cephalosporin and a
Macrolide or if it is a hospital-acquired then you need to cover for MRSA pseudomonas Etc. We talked about NSAIDs already trying to avoid about blood clots. If officially if you go to places like up-to-date at least currently at this point, they do recommend low molecular weight Heparin for prophylaxis. That will be like Lovenox 40 milligrams subcutaneously if they’ve got good renal function, but there are some data that’s come out that has shown that if the D-dimer is elevated,
More than one microgram per liter. There’s about an 18 fold increase in the mortality of these patients. I think that’s a very very strong signal that thrombosis is the is the real problem in covid-19 and maybe the big issue at least I’m feeling at this point. There’s no recommendations for anticoagulation at those levels at least here in the United States. I do know that the UK is
In full anticoagulation in some of these patients and this is what I was talking about before here’s a paper that was published in thrombosis research showing severe covid-19 infection associated with endothelial activation. This is a case where they basically took a patient that had come in during the ICU stay and by day 21 when they check D-dimer levels they were as high as 21 or even higher and that the Von Willebrand factor and the factor 8
was at five times the level of what it normally would be in that situation. And so this sort of goes along that there they say that there was endothelial damage that was causing Von Willebrand factor, you know, I’ll say something that’s very interesting that we are looking into as well that there was some research a number of weeks ago or a month or so ago that showed that type O blood type had a better mortality than type a b or
A bee well, it’s interesting to note that type O blood also has the least generally speaking the least level of circulating Von Willebrand factor now, whether that’s just an association or a coincidence, but I find it interesting that we’re seeing high levels of Von Willebrand factor and clotting factors in this disease, which is certainly endothelial in nature.
Again, angiotensin-converting enzyme to confers endothelium protection and attenuates atherosclerosis here. We see that a stew which is what we were talking about before makes Angiotensin 1 7 and this does helps the the endothelium by attenuating by suppressing nadph oxidase. And so their conclusion. Was that a stew treatment approaches, maybe a novel approach to limit aberrant vascular.
Houses and a thorough thrombosis, so it’s a direct connection here. And if you look at the antioxidant system, you’ll see here very clearly that nadph oxidase makes this super oxide and the superoxide dismutase reduces it back to oxygen or oxidizes it back to oxygen reduces it to hydrogen peroxide hydrogen peroxide, of course is metabolized by the glutathione peroxidase system, which is reduced by things like, you know, n-acetyl cysteine.
Which is being used and Etc. So this the system is
Plugged into if you will be a stew and the Angiotensin one seven system. So I think that’s that’s really important.
Here’s another study that showed that oxidative stress and it says here there’s evidence for the critical role of nadph oxidase derive oxidative stress and atherosclerosis has come from both selke cultural studies and animal models nadph oxidase and superoxide those species that we’re just talking about is increased in vascular cells by a variety of agonists. One of those is guess what Angiotensin 2. So if you knock out a stew like we
Talking about before if you knock out a stew this one right here, which is responsible for metabolizing Angiotensin 2 then instead of you metabolizing it to Angiotensin 1 7 which is a vasodilator. It’s going to be going on this pathway. It’s not going to be taken out by Angiotensin II it’s going to allow the virus to bind the virus is going to take out your a stew and Angiotensin II is going to bind to its receptor and
cause all of this oxidative stress angioedema vascular DM I should say increased blood pressure vascular permeability and all of those sorts of things. So what’s the bottom line there in terms of anticoagulation? I think there may be a benefit to anticoagulation. We just don’t know specifically and that’s why these organizations really can’t say for sure because we haven’t done the studies yet, but it’s certainly looking like this is an area where a Target
Therapeutic Therapeutics. All right. What about oral? What about nebulizers? We don’t want to spread the germs. What about steroids? You know, they say that you shouldn’t start steroids just for covid-19 and that could be associated with increased mortality because of it was an influenza or there could be decreased viral clearance because they saw that in MERS cover as well. We’ve talked about Ace and a Arby’s you can see that very clearly it would seem to say that if we could somehow
ow, reduce Angiotensin II by putting somebody on an Ace inhibitor or block Angiotensin receptor blocker by putting them. I mean Angiotensin receptor by putting them on Angiotensin receptor blocker that that would help. We just haven’t done those studies. So we don’t know for sure. I would say that if you’re on them, I wouldn’t stop them. If you’re not on them. I wouldn’t go and put yourself on them because there are other potential side effects of that. So take it by case-by-case basis.
All right. So let’s talk about some individual medication. So REM death severe it big in the news yesterday and the day before.
It’s a medication that’s been around. It’s been tested It’s relatively safe. It just hasn’t had an FDA approval because it hasn’t worked in anything up to this point. They tried it in Ebola and it didn’t work. What it does is it stops transcription and stops that replicates that we were talking about at the very beginning of this webinar. Well yesterday there were two officially published news articles. One of them was actually a paper in the Lancet and that showed that was a
Of China that really didn’t show any benefit to rent a severe if there were a couple of criticisms of that study number one was that it never reached its full conclusion. They weren’t able to fill the study because the epidemic in China had gone away by the time it was in full swing. The other one is that they could enroll patients that study up to 12 days after they became infected. We know with studies here in the United States and around the world that Tamiflu you need to be on Tam.
Even within the first 12 to 24 hours. So that was a negative study. Unclear exactly what to say about REM death severe. The other study was an interesting study. That’s a study that’s done here in the United States. They originally enrolled over a thousand or that was the goal. But with these studies what they do is they look at them and they see whether or not their endpoints have been made and the two end points that were important in that study was time to improvements and also mortality so when they
The interim evaluation of the study they found that those endpoints have been met and that it was unethical to continue the study and give Placebo to patients when they knew that this was making a difference so they stopped the study and now they’re working on trying to get an emergency use application from the FDA and they’re talking with the maker of R and S severe which is Gilead by the way. I have no stock or anything in Gilead no interest no financial interest as we mentioned.
So they’re looking to see whether or not Gilly I can ramp up production potentially and and get this out there now. I want to make it clear. This is not a cure when you look at the mortality differences in the in the placebo group. It was 11.6% And in the treatment group was a .0% That’s a drop of 3.6% If you do the number needed to treat on that, which is 1 over the absolute risk reduction you get 28, which is what does that mean? That means that you would have to treat 28 patients with covid-19 to save
One person’s life corsets were doing but you can see it’s not like a parachute for somebody falling out of a plane where you just need to treat one person to save their life. You got to treat 28. So it kind of gives you a magnitude of the effect of R and S of are all right real quick. Let’s talk about hydroxychloroquine. A lot of questions about the mechanism of hydroxychloroquine is does it raise the pH of the lysosomes? There’s a prevent binding of the virus. Does it is it a zinc Iona for lot of proposed mechanisms?
It could work by any one of those at this point. It’s been a political football. Unfortunately. And right now we still don’t have a randomized placebo-controlled trial that tells us what I like to do is just quickly go over a video that we did on medcram where we discuss about the different studies and why we are where we are right now.
Princes to hydroxychloroquine people going to ask me about the newest study in hydroxychloroquine. So let’s take a look at all of this. And this is a VA study. It’s a retrospective study. But before we get to this, let’s kind of look at the history of the studies on hydroxychloroquine.
So this is a really good article from good are x.com, which I’ll put a link to and it does a really good job of summarizing all of the different data points that we’ve come across for hydroxychloroquine. The question is what do research studies say about hydroxychloroquine chloroquine and covid-19 course, we know that data is limited but let’s go through all the positive studies for hydroxychloroquine and then we’ll go through the negative studies. So with this kind of started back in would March where there was a report that showed that over.
A hundred people with covid-19 have been treated with chloroquine and their disease was shorter in illness duration compared to those that didn’t but we actually never got the data on this one. Of course, we all remember study number two, which was March 20th 2020. And that was that small study in France and it showed that people who got hydroxychloroquine had a viral load that was much lower than the comparison. The problem was is that the comparisons were between different.
Hospitals the other problem was is that the people who got hydroxychloroquine 23 percent of them had to stop and so they weren’t included in that analysis also six people received as if through myosin which is not even an antiviral. It’s an antibiotic and they got that with the hydroxychloroquine and that combination led to even lower viral loads.
So part of the problem when you combine hydroxychloroquine and is it for myosin is something called can t see prolongation? This is basically the time it takes between contraction of The ventricle and full relaxation of The ventricle. And if that takes too much time, you can get arrhythmias to occur. Then there was a study at the end of March that came out of Wuhan China that looked at cough and fever which had improved about one day earlier for those that got 400 milligrams of
Roxy chloroquine for five days compared to those who didn’t get any additionally pneumonia improved in 25 of 31 patients who receive hydroxychloroquine to 17 of 30 one who didn’t okay. So now let’s look at some of the negative studies in this study the look to see which group kicked the virus faster and 30 people were given either Placebo or hydroxychloroquine for five days and in the placebo group,
Three percent tested negative versus 87 percent of people who receive hydroxychloroquine tested negative after 5 days. Basically, it was a wash
And there is a French study which tried to duplicate what have been done in their country prior with a see-through myosin and hydroxychloroquine, but here after six days eight of ten patients were still positive for stars cup to one person even died. But again, this study didn’t have a control group either.
Here again. They’re looking at a hundred fifty patients to see which one kicks the virus faster this time. They got 1,200 milligrams for three days then 800 milligrams for two to three weeks or not. And at the end of the study 85% of the patients who got hydroxychloroquine tested negative versus 81% who didn’t get the medication or got Placebo. So pretty much these different groups behaved about the same regardless of whether or not they got the medication or not.
Okay. Now we come to this study the study that we’re looking at today, which was the VA study. Now. The first thing you got to realize is that this is a retrospective study. So this is not the highest level of evidence that you can get. But it’s a fairly large study 368 male veterans all of them over the age of 65. So once again, it may not be generalizable, but disturbingly the death rates were the highest in a group that actually received a hydroxychloroquine and
And the next highest in those the got the hydroxychloroquine and was a through myosin, whereas the group that did not receive hydroxychloroquine had the lowest death rate and this was actually statistically significant.
So the thing that’s really interesting about that whole article was that yeah, the patients that had the hydroxychloroquine. I had a higher mortality rate, but those two groups were really different from each other. One of them was a lot sicker than the other and so the question is is those people that died more likely to die that group that was more likely to die. Was it because there are hydroxychloroquine or was it and they were on hydroxychloroquine the same thing what we talked about?
Beginning with in the JAMA article with patients who are admitted to the hospital and placed on ventilators. They had a much higher mortality rate. Was it because the ventilators were killing them or was it because they were dying and they were on the ventilator and that’s the problem with retrospective data as you can’t tell that difference which is why we need to have a prospective study.
The other thing that people are doing our convalescent plasma. So these are patients that have already come down with covid-19. They’ve recovered they’ve gotten antibodies. They donate those antibodies and we give those antibodies to other people who have not recovered. There’s only a few ways you can get this right now in the United States and hopefully also around the world clinical trials is one way. There’s something called an expanded Access program where you your hospital can be plugged into getting that at least in the United States.
You can apply to the FDA and I’ve done this before you write an email to them through their site and they will give you emergency access so that you can get a number and your blood bank who’s hopefully collecting the plasma can then give it to your patient. We don’t have a randomized controlled trial on that at this point. There’s talking Elysium AB, which is an anti il-6, which is implemented in thought in the storm.
Again, we don’t have any randomized controlled trials on that. There’s others right? There’s the VIP. The rear I/O say this wrong feather pair of ear and RNA polymerase inhibitor. There’s interferon beta there’s Le Pen involve a ton of air and all of these really we don’t have any randomized controlled trials on at this point. Wh o is also doing some randomized controlled trials as well at this point. The only one that we have a randomized controlled trial on is actually render severe.
What about hospitalization? So I’ve got some factors here that tell you whether or not the patient should be hospitalized hypoxemia respiratory rate more than 50% of the lung involved High CRP. You can see the rest of the labs. They’re all of these are predictors that the patient should be admitted to the hospital people that don’t need to be hospitalized fever malaise cough. No shortness of breath up-to-date says that they say quote we generally do not treat patients with non severe disease with experimental agents outside of the context of a clinical trial, but you know as
Talked about before there’s a lot of people in that face too. There’s Millions potentially. These are people that don’t even know they have covid-19 perhaps or they have it and they’re just sitting at home waiting to get worse. What do we do for these people? So there’s a lot of things that are being looked at Vitamin D. We’ve got good evidence just most recently out of Ireland that shows that vitamin D supplementation in those that need it can cut chest infections by 50%
vitamin C has some retrospective data with a RDS and also with sepsis care certain in Ebola zinc. We know in vitro inhibits coronavirus. We also know that zinc helps in Vivo as well for other viruses. There’s the BCG vaccine that we talked about. There’s the vaccine itself that we’re looking at an asset sale system, which is a antioxidant for the glutathione peroxidase system that we talked about before there’s even a trial looking at famotidine in very high intravenous doses.
Talked about before I’m a crime about hydro thermal therapy. This is what they used to do a hundred years ago before we had trials and we know there’s good evidence looking at elevated fever can help they did this before with neurosyphilis and by giving patients malaria to treat the neurosyphilis and then treating the malaria. So there’s a lot of good data from many many years ago. They’re looking at doing natural killer cells from placenta mesenchymal cells and infusing those we know that sleep is very important.
Could talk about that for another hour if we needed to and then finally nutrition because what we’re noticing in these patients is that the patients that are being admitted to the hospital. They are very rich on cardiovascular disease BMI hypertension, very low on COPD and Asthma this is actually surprising because we thought these were the people the COPD and Asthma patients that we’re going to be ending up in the hospital. It’s not it’s the more oxidative stress endothelial cardiovascular stress type.
And again here. So here’s the Paradigm oxidative stress moves you to the left and what you see here on the left is the result of high carbohydrates glucose fructose a high saturated fat oxidative stress things, but moving to the right are the things that we see associated with whole grains fruits vegetables Etc. These are the things that are nutrients for the endothelial cells and it could be, you know, a multiple hit model here where these people that are on the left hand side.
And with a lot of oxidative stress and now they’re getting the coronavirus which tips them over the edge. And that’s why we’re seeing people with cardiovascular disease and large BMI is getting into the hospital as opposed to people with lung disease again more evidence that this may be a more complicated disease than we actually thought so in summary working hypotheses patterns are emerging in the hospitalization of covid-19 prognosis is poor for severe patients at this time. There is
One positive randomized control trial remedy severe and that looks promising. It’s another tool in the toolbox. It’s not a cure there’s many interesting leads which need to be looked like looked at not the least of which is the endothelial situation in the vasculature. And of course, we’re going to need more randomized control trials to know for sure. We need to look at thrombosis and of course nutrition and with that I think we’ll open it up to any kind of questions Kyle.
I’ll at this point. Thanks for having me. I’m going to summarize a few questions that I’ve seen multiple times on our YouTube live stream. And the first one a lot of people are wondering about Kawasakis disease and the reports of you know, especially children and Europe getting Kawasaki disease. Could you talk a little bit about that? Yeah. So Kawasaki disease is essentially a vasculitis and that’s that’s what we’re that is what we are basically talking about.
About when we’re talking about oxidative stress on the endothelium we’re talking about if you noticed on on that article where they wrote in on thrombosis, not only did they find elevated levels of factor 8 and Von Willebrand factor, but they also found elevated levels of anti cardiolipin antibody and anti beta beta life and antibodies as well. When you are ripping through endothelial cells. You are exposing parts of the
Vascular tree that should not be exposed and your immune system is going to make antibodies against it and depending on what’s exposed. You can imagine there’s going to be different antibodies. It’s certainly possible that it’s certainly conceivable that in some patients when you have endothelial dysfunction and you expose a parts of the vasculature teary immune system, you’re going to get antibodies against various things Kawasakis is simply an antibody against some of those things and so it’s not too surprising if that is what is going on and we
I know for sure that if that’s what’s going on. That is what we might see.
Quite a few viewers are wondering about Kirsten and you’ve talked about how one of the possible mechanisms for how hydroxychloroquine could work in fighting covid-19 is through a zinc ion of for and we believe that Kirsten is also a potential using kind of for is there do you think there’s value and doing trials and Karis attends, you know of any trials on Kirsten at the moment excellent question Kyle. So so this is the thing is there are studies that show that hydroxy.
Laura Quinn acts as a zinc. Ion of for no question about it. There are studies that show that zinc inhibits coronavirus replicase. No question about it. There are studies that show that care certain is a zinc. I own a for no question about it. There are studies that show that care certain may be beneficial in coronavirus. It has been proven or been shown to be beneficial in Ebola. So
Those are all dots if we connect those dots we come up with a line and that line may be true. The line might not be true. So is it possible that if hydroxychloroquine is a zinc ion for and cares Latinas in kind of for that Kirsten might work the answer is yes, then it’s possible. It’s even possible that care certain is a zinc Iona for and it does it in a completely different way. We don’t know for sure because all these tests have been done in vitro.
And unfortunately, when you do something in vitro, you’re controlling all of the variables except for that one variable. However, when you put that into a system into a human being into an animal at cetera now, it’s playing back and forth with a holes. It’s a very complex system. And so we really don’t know the answer to that. They are studying here certain. However, there’s a doctor. Dr. Cutten in Canada. And another Chinese physician are both
Supposed to be conducting randomized controlled trials in China on Kirsten. And so maybe we’ll know the answer when they get done with their work. Okay, another I’m going to summarize another group of questions that come in about anticoagulants and the risk of myocardial infarction the risk of stroke the risk of pulmonary embolism with covid-19. So for a patient that gets hospitalized at this time what we know now,
Would you put them on anticoagulants prophylactically and if so, what would be one of your first choices to do that? Yeah. So what I’m doing right now is I’m looking at the D-dimer levels and at the D-dimer levels are depending on the scale in your hospital greater than 1 or greater than a thousand depending on whether using Nano grams or micrograms deciliter per liter. Anyhow, I think the current recommendations of what they’re looking at at least out of the UK is to put them on some sort of anticoagulation if
there is no contraindication. I say that slowly because I don’t want to think that everybody needs to go and anticoagulation. There’s a risk in thinning everybody’s blood of course. So you need to look at the risks versus the benefits from the evidence that I have seen or at least not the evidence but the expert opinion Heparin drips are being used. Although the issue with Heparin drip is is that it you do have to titrate it. The nice thing is that there is a bleeding problem. You can always turn it off fairly quickly we
Currently using low molecular weight Heparin in our patients who we believe deserve to have anticoagulation most of the patients that we’re seeing that are sick enough to be in the hospital have d-dimer’s well over one point zero and so that is that is currently what we are doing. We don’t have any evidence for this. It just seems reasonable that if we’re seeing that their d-dimer’s are high and this could be a coagulation issue. It’s reasonable to put them on a blood thinner if there is no danger of them bleeding.
And just to follow up on that player Upper Michigan had a specific question along those lines. She said she had a patient with covid-19 that had a stroke had an acute CBA and is on Xarelto currently how long should she can’t up anticoagulate for? Well, that’s a that’s an excellent question. So I’m assuming she was placed on Xarelto after she had these Strokes not not before it. That’s an excellent question. You know it. It’s an interesting.
Pain because I remember hearing early in this course about patients who are recovering in the hospital and then going home only to come back very quickly and die and it’s like well what is going on here? If this is just an AR DS picture, we don’t see that in a RDS of patients. So that makes me think even more that this is an endothelial dysfunction because when patients present to the hospital and they have a blood clot and that blood clot is due to something that we know.
So in other words, it’s a provoked blood clot. For instance. They were in a car for too long or they were on a plane for too long. And we’re able to remove that provoking Factor. So they’re not going to be on a plane. In this case. It would be that they’re no longer infected with coronavirus. The minimum recommended time for anticoagulation is three months. So I would say at this point if it turns out if it turns out that covid-19 is a hypercoagulable state and the patient has developed a clot and we believe that
Our clotting factors will go back to normal after the infection goes away and all of those are ifs then I would recommend at least it would seem logical that at the very least these patients should be on blood thinners for three months. That’s just a expert opinion that we call that Grady evidence. That’s expert opinion. Got it. Okay one more question about her.
Oh we can we can go as long as we need to go. Okay. So this is a clinician from Ohio that is wondering how to counsel patients aside from promoting good balanced nutrition quality sleep exercise, you know maintaining a healthy weight. What else do you think the evidence is good enough at this point to recommend and is there any reason to discourage these patients from supplementing with vitamin?
D vitamin C and zinc in relatively low doses. Yeah, so long as those doses are relatively safe. There’s no reason right now because of the lack of randomized controlled trials that we just have one at this point and we’re not even able to get that medication. So essentially we’ve got nothing right now. Everything’s got to be benefit versus rest. I’ll tell you what I do. So I do take zinc. I do take Vitamin C. I do take vitamin D. We made a video about it Kyle the other thing that I do.
You know, there’s some evidence that that heat followed by cold can be beneficial. If you look at the Finish data that takes on has they have 50% less respiratory infections. When you look at a an associative study that was published a number of years ago. So hot cold showers all sorts of things at this point, you know, it may work. It may not work. I’d rather be on the side of doing something that didn’t work then not doing something that could have worked.
Excellent and Roger remind you there more to your presentation or we purely in the question answer. We are clearly the question and answer period okay, excellent. So just so the viewers out there that have hung with us this long though. We’re going to go for at least another 20 minutes. And again, we apologize for the difficulties at the beginning but we’re going to keep the question-and-answer going and the next kind of we’ve seen a lot of questions come in about antibodies and about immunity and I know
Lot, we don’t know at this point, but based on what we do know or what you know about coronavirus has Roger. What what’s your feeling about the ability of this Stars Cub to virus to mutate relative to something, you know, we’re all familiar with like influenza.
Yeah, so it’s certainly possible Right. How many times a year do we get a cold? We get it often and this is coming out of the family of cold viruses. So there that being said there was a study that was done Kyle that where they looked at monkeys and they infected these monkeys once with a particular string of the coronavirus and then they try to do it again and they couldn’t do it and that that tells us that yes, so long as the virus doesn’t mutate to dramatically then we should be able to have immunity.
You to it. That’s no surprise. The question is about mutation. Generally speaking mutations should affect the entire genome equally generally speaking. That’s what we should expect but you’ve got to realize that if there’s a mutation in the spike protein, the very protein that is essential for the virus to infect a human that virus is never going to get into that human because of the mutation so we don’t expect highly conserved areas of the
virus to mutate because that’s how they get in to the patient. And so if we form antibodies against that portion of the virus it stands to reason logically that that immunization should be good at least for a period of time so long as the body can make those antibodies, but we don’t know until we actually get the virus and get the vaccine out there and then along those lines seen a few questions come in about MERS and SARS.
And people that have had those particular infections. Do we have any reason to believe they might have a community or a less severe course of covid-19. Yeah, it’s possible. Although the amount of people that were talking about is is minuscule compared to the number of of SARS cup of to patients. But yes, the tsar’s one virus or just the SARS virus as we call. It had had the same receptor the Ace 2
ER as its Target and so it’s very possible that if antibodies were formed against ours that those antibodies, you know, 10 years later may be effective against ours cup of to but it’s you know, you and I both know and I me as a medical doctor used to be a medical student and we used to have our titers check. I remember I got immunized against Hepatitis B as part of my medical school matriculation and years later when I had my Hepatitis B titers check
They were negative. So I had to get a booster and so it’s possible, you know, the Stars was 10 years ago or more 20 years ago actually and so it’s certainly possible that those antibodies have burned out excellent. What about Ivermectin lot? A lot of folks have written comments about Ivermectin did that just kind of fall off the map or or I should have probably included it in the presentation. So Ivermectin is an
he parasite medication. We usually give it once to patients that come into the hospital. It’s very it’s a fairly benign medication what it is what it does is it prevents the transport of viral proteins into the nucleus. So there’s a viral there’s a nuclear transport mechanism that transports things from the cytoplasm into the nucleus of the host cell and the virus uses that transport mechanism to
And support its proteins into the nucleus to prevent the cell from replication from doing various different things if that’s an immune cell. There’s certainly going to be problems with immunity. What Ivermectin does is it shuts that transport system down temporarily and prevents the virus from suppressing the immune system, at least that’s what it’s felt to do at this point. You can give somebody Ivermectin and it usually lasts for about a week. We usually do sit another week later if that’s what we need to do but a very little
Has side effects I’ll tell you the patients that I’m seeing in the hospital. They’re getting hydroxychloroquine. They’re getting zinc. They’re getting high dose vitamin C. They’re getting Ivermectin. They’re getting if they have a high D-dimer. They’re getting Lovenox. They’re still very sick. They’re not like dramatically improving the next day. I have not given any of my patients rammed a severe because I haven’t had it available. It’s very difficult to get the only way you can get it right now is on a compassionate use for people who are pregnant.
It’s more for Pediatrics right now. If you’re not pregnant and you’re an adult’s the only way you can get it is through a trial or wait for the FDA to get that emergency use that we were talking about. So I’m seeing a lot of questions come in about nitric oxide. Yeah have any information on that to share. So nitric oxide is basically a way of dilating the vasculature and so Angiotensin II as we talked about is a vasoconstrictor. It constricts the pulmonary.
Vessels potentially could also cause thrombosis. So if that Angiotensin II is constricting the blood vessels in the lungs particularly in by alveoli that are ventilating. Well, it would be very beneficial for oxygenation purposes to dilate those pulmonary arteries permanent arterioles capillaries that are next to the alveoli to allow more blood to Flow by ventilated alveoli. Well if you’re breathing in nitric oxide
No, that that nitric oxide is going to go to well-ventilated alveoli. And so they’re actually proposing a study to look at this to see if they could even get patients not only to have better oxygenation. But to send them home the trick is in getting a device that they can take home with them and to getting a medication that is long-lasting enough. So that the patient doesn’t have to do it more than four times five times a day. But yeah, that’s a very interesting and promising looking study that may be beneficial.
Danny from Rhode Island has a practical question wants to know why do you think we’re calling a social distancing? Should we as a nation and as a world be calm it physical distancing. Yeah, that’s that’s an excellent question. And you know what? I didn’t even think about it until someone had brought that up. They called it social distancing and so I called it social distancing but then when it was brought up to me actually was you Kyle that brought that up to me and made me think about that. We shouldn’t be socially.
Since in ourselves, we should be socially connecting ourselves at this point the real key see that the virus doesn’t spread by social communication connectivity. It’s by physical and so we should be doing physical distancing but what we’re doing right now with you there in Rhode Island, and with the people in the in Australia and the UK and India is we’re getting together and it’s fun to do that. And I’m glad that we’re here so we should not socially distance our audience know
So a lot of questions coming in about and I know Roger you did a video earlier on in our covid-19 updates about how much the how many mutations have already been observed in source code to and we hope relatively minor mutations. Of course, there’s some speculation that maybe places like New York places like New Orleans that had a really have had significant outbreak may have a more severe strain and other parts of the country.
Can you talk a little bit about in the context of a vaccine which we’re all hoping? We have big a difference between minor mutations that a vaccine or previous infection would work for versus a large-scale mutation. That’s that’s big enough to actually render a previous infection or vaccine not effective. Yeah, that’s that’s a real concern.
Kyle that that is a real concern because we’ve seen that we see that all the time with influenza, which is a different virus. It is an RNA virus, but it it looks like a completely different receptor and so you can have shifts and you can have minor tweaks and and depending on what you get. It’s going to be a completely different type of infection, right H1N1 2009 swine flu. That was a major major epidemic. Could you see something like that that way with SARS? Yeah could Stars join?
Our qadri of seasonal viral infections. It’s certainly possible and would a vaccine help. Yeah, we could be dealing with the same thing that we’re dealing with with the influenza will always looking ahead to Australia to see what kind of infections are going on there and try to get it predicted correctly here. So it’s certainly possible that is not outside of the realm of reality the website. I think that’s very good on that is next rain which which
each tracks this coronavirus and all the different viral strains. There’s some feeling that the New York strain was it was obtained from Europe and that’s the California strain or the West Coast Reign was was gotten buy directly from Asia because of travel patterns, of course, you know, whether or not one gives you immunity to the other Still Remains to be seen. I think it’ll be interesting to see if that’s the case.
Okay, I’m seeing a lot of questions about trials and where do we stand and kind of taking a step back and look at the big picture? What are the next steps in combating covid-19. So this is putting me on the spot here Roger if you had a grant for a significant amount of money and you could design a study a trial, however you wanted to
With whatever medications or supplements you wanted to what would be one that would, you know kind of rise to the top that you could initiate down there in Southern California. For example, well, this is more of a philosophical question because I’m sure that there is a perfect anticoagulants probably out there somewhere that we could use and will be great to try that. It would also be great to find out how we could eliminate some of this endovascular problems. I think that would be a great trial ivory.
It looks like a great trial the all of these trials look good hydroxychloroquine would be great to have a doll being done at this point and eventually they’re all going to come out and but the question really remains is what I was talking about before which is phase two the real issue here. Is that by the time you have the farther down the course of the disease you go. Okay hospitalization intensive care the less you’re able
All to actually change on this patient that makes sense. Right? Because the there’s been more time for the virus to do what it needs to do whatever it’s doing but there’s also less people to treat and so it’s easier to make enough of a medication to treat that many people what I would like to see what I think would be amazing is to find out further up the course. Is there something that we can do to reduce the progression?
In those early days of the infection something that’s very simple something that doesn’t require a drug to be manufactured for instance something that doesn’t require a distribution or logisitics to get out. All it takes is information and understanding and if there’s something that we could do at that time whether it be dietary things like you talked about nutrition whether it be what we
Saw maybe a hundred years ago in these sanitariums that we talked about if we actually knew what the effect of that was and we implemented public health strategies that could be very helpful in preventing a lot of hospitalizations. And if we were able to mitigate that if it worked it would be able for us to open up Society potentially and to be less restrictive because we wouldn’t be worried about flattening the curve and having that bar. So low, so I think from a public policy
Points if I had unlimited source of resources, it would be instead of focusing my energy on phase 3, which is hospitalization. I would love to know the things that would really work in face to that could bring down the the progression of this disease in other words if 80% are getting better and don’t need hospitalization. What is it about that 80% Let’s make it 90 percent or even 95 percent that would to me be the biggest win that we can have.
Okay back to a testing question here Roger. If someone’s had a positive covid-19 test the PCR test for acute infection. They recovered they’re no longer showing symptoms. Are they okay to go back to work and if so, how long should they wait before going back to work whether it’s in health care or some other industry. So I think you’ve not understand that those negative PCR.
Are potentially depending on which one is done plagued with false negatives. So depending on how critical the job is for instance. If you’re a health care provider, are you going to depend on one negative test? You know, some would say no you want to if you’re a nursing home and your and you are accepting a patient back to your nursing home. Do you just want one negative test or do you want to so this is this is what we’re talking about here. Is it really depends on how critical is it?
It that the patient really really be negative. If you’re just going back to your home and you’re just going to stay in your home. Anyway, maybe one negative test is is as fine. And that’s why I think you’re seeing differences in terms of the situation about how many tests are required here. How many days being symptom-free here? It’s being tailored based on the on the clinical situation. So if it’s a very critical period where you can potentially be a super spreader, we’re going to really want to make sure like if you are a healthcare worker and you can spread it to a lot of people
Our immuno compromised you’re going to really want to make sure that these patients are protected and that that person in particular really is negative for coronavirus. Okay a question from Mary Lou and Scottsdale, Arizona and Rocky talked about this in some of your previous videos, but we know that the rate of infection and a Severe covid-19 is lower in children. I take that back. I don’t know if the rate of infection is lower, but we know the city.
Charity overall is lower in children. How do you make sense of that? Well, one of the proposals that has been put out is the innate immunity. So the innate immunity that wing of the immune system which basically goes around and just eats things up and then presents it to the adaptive immunity is very strong in young people and it gets generally weaker and weaker as you get older and older and so anyway that an adult can strengthen their innate immune system is
Something that is worthwhile doing there’s a number of things out there that we’ve shown that can do that. Just there’s been some studies that show that by increasing the temperature sitting in a hot bath for a period of time to raise the temperature. They took monocytes out of people who had done that subjects who tested that those monocytes were more plentiful and actually had a more effective response against lippa polysaccharide, which is a bacterial chemotaxis that so
So the we know that fever is the body’s innate immune response, right? And we know that kids when they get a viral infection almost all of them get fevers. Look at the study that we just did showed there in Jama what percent of patients with covid-19 came into the hospital with the fever 30% 30% when I went to the hospital today, there was someone standing at the door that was checking to see who was coming in and they were doing these scans on your head to see what
Temperature was just realize that seventy percent of the patients that ended up at the hospital with covid-19 did not have a fever and so that is part and parcel of of the innate immune system getting worse as you get older.
Okay question about aspirin and we talked about anticoagulation. We’ve talked about risk of emboli and myocardial infarction and and a stroke. Do you think there’s any compelling reason to take low-dose aspirin, you know, even for an adult it’s you know, not over 65 years old in the setting of a pandemic like this.
The concern that I have is that taking low dose aspirin May impair your body’s ability to mount a fever.
The other aspect of this is that aspirin predominantly affects the platelets. Okay, whereas in covid-19, a lot of the negative factors are mitigated by hyper coagulation. So actually the coagulation factors. Of course, I’ll be it von Willebrand’s is involved with platelets and coagulants kind of that bridge between the both. We just don’t know and I’d hate for people to be put on.
Low dose aspirin. I mean there’s a lot of risks and putting a lot of people in low dose aspirin when it comes to ulcers in the stomach and and inhibiting your platelets also inhibiting fever as well. So this is I think a discussion that you have to have with your physician. What about hyperbaric oxygen, you know, you’ve explained today and in your updates about you know, how this hypoxemia
can be a result of her can occur in patients with good lung compliance. Do you think hyperbaric oxygen is something worth trying do you know of anyone that that’s currently studying that so hyperbaric oxygen is a way of instead of if you go to a hundred percent oxygen on the ventilator that’s 760 millimeters of mercury. That’s as high as you can go. You can’t go any higher than that, especially if you know, that’s at the sea level, right? So a hyperbaric oxygen if you go to
And a half atmospheres that allows you to get a tremendous amount of oxygen through the barrier through the alveolar barrier and into into the blood. The problem is that to get somebody those different types of hyperbaric chambers. There’s ones that you can literally walk into those are very rare. Mostly what you see is these little cylindrical tubes that you fit very closely and while it is possible to get people in there on ventilators.
It’s very difficult to do that. And there’s probably just not enough of those. Theoretically I imagine it might help with the oxygenation issue, but there’s a whole bunch of other issues that brought get brought up when you’re dealing with hyperbaric oxygen not the least of which is that a lot of these patients are unstable there on days oppressors. These are medications that are used to increase their blood pressure. And if something were to happen to that patient in the tube, you’ve got to wait a particular period of time maybe 20 30
Some cases to bring that pressure down slowly. Otherwise, you could have what they call the Benz, right? You could have Micro bubbles that could cause embolisation and make the situation worse. So it’s difficult difficult situation that you I think probably a more practical way of doing is ECMO, which is where you actually just bypass the heart and the lungs that also is difficult because of the limited amount of echo echo is not without its drawbacks it can cause
Any strokes and things of that nature so depending on on if things embolize so it’s not risk-free at this point, but certainly something that has been done ECMO that is okay another question about recovering from covid-19. And of course to this point, we have a lot of patients that had covid-19 and have been given the title recovered. So two part question, how much do we know about how the definition of a record?
Upper cover patient in different countries all over the world. Is there standardization to that and in a future pandemics? Hopefully we ever have one if we do, you know, should there be more leadership about getting a good definition that each country is following so that we’re consistent with that. So I’ll start with that question. I have a follow-up after yeah, so there isn’t a definite definition of what quote recovered means generally it.
Usually involves a negative test. It usually involves being symptom-free for some period of time but all of those things differ those at one test is to test is at two weeks is a 10 days all of those things are different, you know in these diseases that we study when we have time to do it for instance a RDS. We had a Berlin Conference and they have the Berlin criteria where the whole world gets together and says, okay, we’re going to study this disease and here are the definitions of the disease that we’re going to have.
You know we never had time to do that part of the problem with covid-19 is that you couldn’t travel so that was the last thing that they were able to do. I don’t know of any International Conference that has happened other than what the who is doing in terms of standardizing. What does it mean to be recovered? They may have those definitions, but I know politically because countries want to manipulate numbers potentially. They may change the definition of what it means to be a case to be a suspected case.
To be a recovered case to make their numbers look better the same but certainly at this point, we’re not we’re not there as yet. Okay and along the lines a lot of viewers are asking about the sequelae of covid-19. If someone gets covid-19 and they they’re no longer symptomatic. What do we know and is enough being done to study the sequelae in these recovered patients from covid-19.
Yeah, so that’s a very good question people who have strokes people who might have had fibrosis in the lungs. I know there’s a study that’s looking at n-acetyl cysteine with recurrent fibrosis or fibrosis as a result of the infection about this whole thing about oxidative damage and and following those patients. I think it’s a great question right now. I think we’re trying to get our head wrapped around how to get out of the epidemic people will be looking.
At this there’s no question about it. I think we’re about at our time for the live stream. Any parting words project. Yeah. I just wanted to thank everybody around the world for joining us. I know that there’s people in all over the world and I want to know that we really appreciate all of the comments that we get. We cuddle and Kyle and I read all of the comments and we we can’t respond to all of them, but we really appreciate it as I was telling
While a number of days ago really a lot of the ideas that we get an order what to follow come from a lot of the comments that you guys give. So we really appreciate this. We don’t feel in any way that learning is going here in One Direction because it’s definitely going in two directions and I really appreciate the fact that you have all stayed on and listened and watched and I really want to thank also continuing education company for hosting this this is a this is a work in progress, but they’ve they scrambled
I did a great job based on the the barriers that were kind of thrown in the way here at the last minute. And so it takes a lot to sort of knock us down, but we’re here and we’re on the net and we’re thank you. They all joining us. Well, thank you very much. Rob you’re going I’ll I do have a couple of questions for the two of you. So you’ve been putting up these medcram. Excellent. Medcram covid-19 updates on a regular basis. How long do you think you’re going to continue? When do you say? All right. It’s time to stop.
That’s a great question. Kyle says are you up for another video Roger? I said sure, you know, you know Walter and Kyle both. I’m I’m in the thick of covid-19. I’ve saw patients this morning and I’m currently still seeing patients in the hospital for this I find for myself personally that if I have to learn something I want to learn it as if I’m going to be teaching it and so this has forced me this.
These videos every night has forced me to stay on top of a situation. That is very the say this all the time. It’s very fluid. It’s emerging. It’s evolving all the time. And I think doing these videos of actually made me a better physician and treating treating these patients and Kyle. I don’t know I can speak for myself. How about yourself? Well, we’re not too far away from a hundredth day. So I think I think that’d be a good goal. But hopefully that the pandemic is behind us by and we don’t need to go that far.
But great. Yeah. I know. It’s been it’s been great working with you. Dr. Swell and I hope to continue these updates as long as we need to. Yeah, so we know that we had some technical issues early on when we started we started a little bit late. I want everyone to know who is watching that we plan on getting these videos up or an actual video of it without the technical problems cleaned up and we’ll send it over to medcram so they could post it for their viewers and it’ll be on the continuing education website. See I’m eating
Org as well and we hope to get that actually tonight in addition our Kyle and Roger. I’d like to give you an opportunity to say a few words. If you don’t mind about some of the other videos that you’ve just released that are somewhat related to covid. Dr. Swann was one of my instructors during my physician assistant training at Loma Linda University. And the the first lecture I got to see dr. Schwab did with his medical acid-base so
That’s a topic that totally confused me. And that’s when we have on our website that I really appreciate. The other one. I love personal favorite is the ECG interpretation explained clearly. We have a lot of other topics vasopressors dka acute renal failure.



Add comment