Update 99: Long Haulers – Lingering & Long-Term Symptoms After COVID-19
Medcram.com welcome to another medcram covid-19 update. One of the things that a lot of people are thinking about lately is getting back to school. And of course, this is a big topic about whether or not it’s safe to go back to school. We’re not going to weigh in on that today. But we are going to weigh in on today is a new idea that might make going back to school more of a reality and that has to do with testing and I want to thank the folks over at
Were at this week in biology which put together a great podcast that they do every week and we’ll put a link in the description below to their podcast and this last week. They had someone on from Harvard to discuss a new idea that I think may actually be a step in the right direction and the question really boils down to testing do we need better tests or do we need more of tests? That maybe aren’t so good, but just more of them.
And that’s really where the question boils down to and it’s a really important question. Especially now that we’ve essentially inundated our current testing capabilities and we’ll get more to that. But before we do we’ve got to sort of review a little bit about how the virus behaves in some of the numbers that we use to track it. So, let’s talk about that first.
So there was this paper that was published in the New England Journal of Medicine that looked at SARS Covey viral loads in upper respiratory specimens of infected patients. And I want you to notice something here. These are all different patients and they’re looking at for instance nasal swabs throat swabs and then they looked at something called the aggregated CT value. So this is something that’s really important that I want you to understand here are the days since onset of symptoms on the x axis starting off at zero and then they have something called the CT value.
So the CT value is a way of measuring the viral load and for every 3 if you went from 40 down to 37, that’s a movement of three points on the CT value and you’re actually going down in value from 4237. But that movement of three actually translates into a tenfold increase that’s right increase in the viral load and so in fact
T values are inversely proportional to viral loads as you go down and see T value you go up in viral load. And so if you were to move about 9 to 10 points, that would be 3 times 3 and so that would be not 10 not a hundred but a thousand times larger so you can see going from a viral load. That’s very very low here at 40 going to a viral load perhaps in the billions or even trillions as you get up to 15 10 or 5. So that’s
something to keep in mind that CT values that are low mean that there’s a lot of virus particles and CT values that are down here in the 40 range are almost undetectable. I bring that up so you can understand because the rest of the discussion is going to be around these CT values.
So let’s take a look at the natural history of a virus specifically coronavirus in this case. What typically happens is the virus starts infecting and there is exponential growth and then as it tapers off the viral particles can actually last for some period of time before they taper off to 0 and again those CT values. This would be around 40 we can go all the way up to five up here. I think the key.
Key number that we’re going to need to look at here is around 35 and of course that can go up and these are approximate values. What we have right now is we have something called reverse transcriptase PCR rt-pcr and we’re going to put that in green now real-time PCR or reverse transcriptase PCR is pretty expensive the gold standard stuff. It’s about $100 a test right now. We’re experiencing pretty long turn.
Times anywhere from 3 to 4 days all the way up to I’ve seen it as high as nine days to get that test back and there’s not that many of them, but it’s very sensitive.
Let’s say just for argument’s sake it’s around 35 CT values. So that means it can detect all the way down to 35 or even as low as 40.
That means that we’re able to detect using reverse transcriptase PCR all the way out to here. And so all of these patients if they were to test would test positive on this test now apparently there are some tests that are known as paper tests and apparently all you need to do with these paper tests because their paper coated with monoclonal antibodies that can detect antigen.
They’re not detecting actual RNA but antigens these are more along the lines of one to two dollars each, but they’re not as sensitive. Some would say that there maybe even 50 percent sensitive now. It’s not a random 50% sensitive. No, it’s maybe somewhere in this range.
So that this is the range of people that we’re talking about.
So the other words here to here and the CT level that we’re talking about is in the low 30s.
And these numbers may be a little bit different but you’re getting the idea of what I’m talking about. One of the things that has been made clear to me is that the threshold of transmissibility is actually more narrow than we thought it was. Well, this is exactly what dr. Mina from the th Chan School of Public Health at Harvard University was making a point of on this week in virology. So people who are
hitting probably have CT values that are below 30 and the vast majority probably have them below 25 or so. How do we know that do we have evidence that people are still positive but they’re not transmitting the virus and the answer to that is yes. If you look back at one of our updates we highlighted a South Korean study where these people that kept on testing positive were checked and they looked at
Household members and they were found not to be infective. In fact, they did background checks and these patients and found that not a single case of transmissibility occurred in these patients that were persistently positive. And the reason is because the nature of this test rt-pcr is you’re looking for fragments of RNA and fragments of RNA while they will turn the test positive fragments of RNA are not enough to actually cause transmissibility. A lot of people are saying
Well, we need the really sensitive tests to to be able to detect people early on in their infection. But almost all of the time that people spend with this virus near the limit of detection of PCR is on the tail end of their infection. This is a virus that once it hits PCR positivity levels. It’s growing well and it’s exponential phase and it’s probably a matter of hours not days before it passes the threshold to be detected on some of these slowly.
Or sensitivity assays and then it will sort of persist for weeks potentially or months even in some people at very low RNA levels. So it’s it’s after people are well beyond their transmissible period that we’re actually seeing the loss insensitivity of these assays it’s very rare that you that you actually detect somebody with a CT value of 39 in that window on their way up because they’re only sitting there for a few hours before they get down to a 33. So if
You’re missing CT values of 39 in my perspective who cares it’s really not that important. And so the point here is that yes these tests here may actually be maybe 50% sensitive but in comparison to what it’s in comparison to a test that may be overly sensitive. And so in fact, the question is is if your threshold of transmissibility is closer to this threshold of actually being positive on these much cheaper tests. These are test the
be repeated on a daily basis and so these tests may actually be more beneficial in terms of controlling and outbreak of the virus because you’re able to do it more quickly and by the way there’s one thing I forgot to put down on here you get the results back in 10 minutes you can have them at home you can test see really maybe once a day maybe twice a week three times a week and if your child is positive then you hold them back from going to school if they’re Negative they go to school and you have real-time
location of this what the CDC is was recent announcement may be his last week 9 out of 10 people go undiagnosed with this virus today in the u.s. I would say that of those men of those one out of ten that do get diagnosed almost all of them are getting diagnosed through surveillance after they’ve been infectious because their CT values we’ve seen the average CT value kind of creep up to 35 or so so that means they’re almost all at the Talon
So what that tells me is if we take a step back and we look at this virus in our testing program in the states. We’re using a very sensitive test, but our sensitivity to detect infections is probably below 5% you know across the u.s. Right now. It’s the CDC says it’s 10% and if we actually say detecting transmissible infections were woefully under you know under utilizing testing. So if we know that Viral the virus
Schmidt’s once people are above say a hundred thousand or million copies per mil.
Then maybe we only need a really crappy test if we can use it. If it’s cheap enough to use it very frequently then if then it doesn’t detect less than 5% of people when they’re transmitting maybe it detects 85% of people when they’re transmitting and that’s a huge win over what we have right now. And if you want to read the preprint of dr. Mina’s work, we have a link to its PDF in our description below. I think he makes a good case for this and I like you too.
Read it for yourself to me. The short way to say it is if the test isn’t as good but we do it every day and you get the results quicker. You’re going to be way ahead in the long run. I mean, that’s the other thing we haven’t really touched on is the turnaround time but the sensitivity okay, maybe not perfect but test every day get the results quickly and if you test wrong the day one on day two
you’re probably test positive you know that’s a that’s exactly right and on aggregate you’ll drive the are effective you know this virus way down below 1 I mean I think if you were to take this and give everyone in Miami or Austin or wherever their burgeoning outbreaks right now now give everyone a test or give 50% of the people of test you would probably Drive our effective down overnight you know if everyone tomorrow could wake up test themselves you’d immediately
we filter out
Tens of thousands of people potentially who are who have the virus in them that day and it the other the other consequences you don’t have to worry about contact tracing because everyone would be doing their own test every day it just you know, it can be done and this is with a pinprick right for a little bit of blood. No. No, this is with a that’s a different thing which I could talk about is the serology but I know this is actually just kind of spitting on a paper strip or taking a cute.
Chip and putting it into a little plastic tube of saline and drawing a paper strip. And then I’m thinking about school kids you get up in the morning and take the test. It tells you whether or not to go to school. That’s also whole problem. Yep, and it doesn’t need to be perfect. You know you have okay, so you have one kid who tests a negative and you know, they actually go to school. Well that kid, you know, otherwise that kids not going to get tested at all, you know, so they’ll find themselves positive the next day and they’ll infect overall fewer people and anyone that they
In fact will on average find that they have been infected and they’ll stay home. So it’s very quickly compounds into a massive reduction of virus in the population very quickly the FDA and the CDC and the NIH have to change their messaging. They have to say look there is actually a technology that a test could exist right now. I have some sitting in my office next to me. They’re paper strips. They’re just little pieces of cardboard prick.
Inted with monoclonal antibodies that can pick up an antigen is essentially a lateral flow sa can be printed in the millions and you may be thinking well, why didn’t these tests come out earlier? Well, in fact they did but they were kind of beat up because of the low sensitivity and this was the paper that did the beating up. This was at a New York University Grossman school of medicine. And if you go to the end of this print you can see some of the
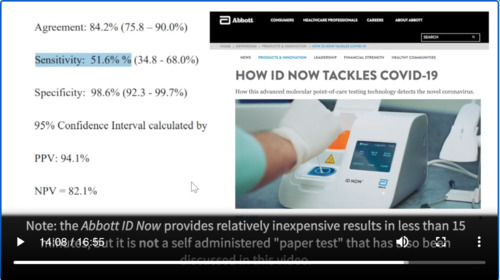
Things that were highlighted in terms of which tests had negative results when the rt-pcr had positive results and you can see here the sensitivity of this test called the Abbot ID now, which is one of these cheap tests that can get done pretty quickly. It had a sensitivity of only 51.6% But again as we showed the 51 percent sensitivity was not just I random 51% the test that it missed or
probably those patients that were passed their infectivity in terms of CT values and more specifically. What is it going to help somebody if it takes eight or nine days to get back a very accurate test, but now they can’t do anything about the results here are this is a very quick test you get it back in 10 minutes. And as you can see here, the positive predictive value was 94.1% which of course would change based on the prevalence. But if you look at some of these tests that were done you can see
Here that we have the cepheid result, which is the gold standard in this case. And then you have the Abbott ID now result which had the lower sensitivity. If you see here this was negative when this was positive. What kind of a test result is it being missed on it’s looking at the nuclear capsid CT which is around 43. That’s an extremely low viral count and probably not going to make a big difference in terms of whether that patients isolated or not. Here is another one at forty point seven.
Again, not a big difference at such a low viral load here 44. Here’s another one forty four point three. Here’s another one at 36.3 where as you can see the higher viral load counts based on the lower CT numbers 29.7 27.6 19.7 18.6. It’s all picking these up. And so what you have here potentially is a test like this. That’s pretty cheap that you could pick up you could test daily find out whether your infective and if you were
I could stay home and prevent infection to other people. This may be a way potentially to get out and get kids back to school which is obviously the ideal situation one of the reasons that dr. Mina points out that the reason why we’re not seeing these as much is because these companies may be having a little bit of difficulty in terms of thinking that they’re going to get this passed FDA approval because the FDA really wants to have some rigid standards in terms.
Of how accurate the test is going to be and if they’re working on that it’s going to raise the price of these tests and they believe that if there is a viral particle in the patient the test should turn positive when in fact the practical definition of what we’re really looking for here when we’re trying to curb and outbreak is who is infective and who is not infective and that may be a completely different question than who has the viral particle and who doesn’t have the viral particle. Ideally what you want is a
they very cheap test that everybody can self-administer that is widely available that will tell you whether or not you’re infective. Thanks for joining us.



Add comment