Hydroxychloroquine Update; NYC data; How Widespread is COVID-19? (Lecture 60)
Medcram.com wasn’t another medcram covid-19 update.
Daily new cases in the United States seem to have plateaued.
Number of daily deaths are kind of all over the place and probably represent different Foci in the country going off at different times.
In Canada daily new cases are also kind of plateauing.
Daily death seem to have peaked and maybe coming down.
The United Kingdom looks very similar to the u.s. In terms of the cases are plateauing. Here’s Australia’s daily new cases. Definitely come down quite considerably and of course since they’re like the southern hemisphere their season would be like October at this point. And so they’re certainly headed into a flu season and this is the place that we’d want to watch first to see if there is a seasonal recurrence.
While we’re at it, we’ll look at New Zealand as well in terms of their daily cases. Definitely have come down considerably.
And the number of daily deaths is almost non-existent at this point.
Had a difficult day in the ICU today had a patient with bilateral pneumothoraces. Basically a collapsed lung on both sides that we had to put emergent chest tubes on you can see me there with what they call a papr which is a positive pressure helmet that goes on your head and filtered and it has to do with how long you’re in there for you can see the other two nurses had just regular n95 masks on which was perfectly appropriate. They were just hooking up the chest tube there at the end. Normally I go in with a regular n95 mask but in
Case of doing procedures they want us to be wearing Peppers. There was a study that was published out of USC and the Los Angeles County Health Department, which differs a little bit from the Santa Clara County study out of Stanford. As you know, we covered the Stanford paper where they came under Fire for the false positive rate may be interfering with their actual positives and also the way they recruited this was a little bit different.
This study that was conducted here in LA County.
So what they did was they sampled from April 10 to 14 a total of 863 random samples at six testing sites and they actually used a professional group to make sure that the sample was as random as it possibly could be in other words. They didn’t use Facebook to recruit.
And the doctor in charge of the research, dr. And Raj stood at USC said he was confident in the Integrity of the LA County tests and that researchers were accounting for any false positives and negatives. He also cautioned putting too much weight into the idea of a reduced mortality rate. Now, why would they think there might be a reduced mortality rate? It’s because of the number of people that they found that were positive for the antibody tests.
They thought that between two point eight and five point six percent of the County’s population have been infected at some points and that this would put the preliminary estimate 28 to 55 times higher than the 7990 for confirmed cases at the time of the study.
So when you have that many people more that have the disease it makes your case fatality rate drop. He says that that rate under the new findings Falls drastically from where it was hovering around 4% But at the same time, he also notes that if only 4% of the population is infected while there’s another huge amount of the population that still potentially can get infected and that means of course hospitalizations and ICU admissions.
So they’re going to be testing for the next three months and they’ll see how things go, but it seems as though and this is not that surprising the amount of testing that we’re doing is way low and that this virus is spreading many times faster than our ability to test for it. It appears how much more is still to be determined this County USC study seems to indicate that it might be on the higher end.
Some interesting things that they found also in the study is that men appear to be more likely than women to contract the illness six percent versus two percent and in the study, they found that eight point two percent of Asians seven percent of all the African Americans had contracted the virus six percent of whites and 2.5 percent of Latinos. So, why are men more likely than women to contract the illness?
Well, there was a article published last week in GQ that try to answer that question. Why does coronavirus disproportionately kill men? And actually I was asked to contribute to this article and it does go through some interesting hypotheses as to why that’s the case and we’ll link to it in the description below if you’re interested, but basically it boils down to innate immunity typically stronger in women because they have two X chromosomes and that is where a lot of the immune genes are.
concentrated among others also the virus tends to affect those with cardiovascular disease which men have an abundance of
Also, let’s face it men we like to go to the hospital much later than we should and in this kind of a situation when you do that it makes it more difficult to treat but as I said here the differences between men are probably greater than the differences between the average man and the average woman so I don’t want men to come away with the impression that because their men they have an insurmountable Hill to climb with covid-19. It’s definitely solid time to examine lifestyle choices.
Which brings us to hydroxychloroquine people have been asking me about the newest study in hydroxychloroquine. So let’s take a look at all of this. And this is a VA study. It’s a retrospective study. But before we get to this, let’s kind of look at the history of the studies on hydroxychloroquine.
So this is a really good article from good are x.com, which I’ll put a link to that. It does a really good job of summarizing all of the different data points that we’ve come across for hydroxychloroquine in the question is what do research studies say about hydroxychloroquine chloroquine and covid-19 course, we know that data is limited but let’s go through all the positive studies hydroxychloroquine and then we’ll go through the negative studies. So this kind of started back in mid-march where there was a report that showed that over.
A hundred people with covid-19 have been treated with chloroquine and that their disease was shorter in illness duration compared to those that didn’t but we actually never got the data on this then of course, we all remember study number two, which was March 20th 2020. And that was that small study in France and it showed that people who got hydroxychloroquine had a viral load that was much lower than the comparison. The problem was is that the comparisons were between different.
Hospitals the other problem was is that the people who got hydroxychloroquine 23 percent of them had to stop and so they weren’t included in that analysis also six people received as if through myosin which is not even an antiviral. It’s an antibiotic and they got that with the hydroxychloroquine and that combination led to even lower viral loads.
So part of the problem when you combine hydroxychloroquine and azithromycin is something called QTC prolongation. This is basically the time it takes between contraction of The ventricle and full relaxation of The ventricle. And if that takes too much time, you can get arrhythmias to occur. Then there was a study at the end of March that came out of Wuhan China that looked at cough and fever which had improved about one day earlier for those that got 400 milligrams of
Roxy chloroquine for five days compared to those who didn’t get any additionally pneumonia improved in 25 of 31 patients who received hydroxychloroquine to 17 of 30 one who didn’t okay. So now let’s look at some of the negative studies in this study. They look to see which group kicked the virus faster and 30 people were given either Placebo or hydroxychloroquine for five days and in the placebo group,
Three percent tested negative versus 87 percent of people who receive hydroxychloroquine tested negative after 5 days. Basically, it was a wash
Then there is a French study which tried to duplicate what had been done in their country prior with a see-through myosin and hydroxychloroquine, but here after six days eight of ten patients were still positive for SARS cuff to one person even died. But again, this study didn’t have a control group either.
Here again. They’re looking at a hundred fifty patients to see which one kicks the virus faster this time. They got 1,200 milligrams for three days then 800 milligrams for two to three weeks were not and at the end of the study 85% of the patients who got hydroxychloroquine tested negative versus 81 percent who didn’t get the medication or got Placebo. So pretty much these different groups behaved about the same regardless of whether or not they got the medication or not.
Okay, and now we come to this study the study that we’re looking at today, which was the VA study. Now. The first thing you got to realize is that this is a retrospective study. So this is not the highest level of evidence that you can get. But it’s a fairly large study 368 male veterans all of them over the age of 65. So once again, it may not be generalizable, but disturbingly the death rates were the highest in the group that actually receive the hydroxychloroquine and
And the next highest in those that got the hydroxychloroquine and the azithromycin whereas the group that did not receive hydroxychloroquine had the lowest death rate and this was actually statistically significant and we’ll go ahead and link to this in the description below but you’re probably wondering how could this even be? How is it possible that hydroxychloroquine actually increase the death rate? Well, the thing that you’ve got to remember is that this is a retrospective analysis and anytime you do.
In a retrospective analysis. There are a lot of things that can come in and mess up the results unless you’re ready for them. Unless you understand that they’re there because things that are associated with things can actually change the way you view some of the results. So here’s the publication of those values you can see the p-value was 0.003 and here in the hydroxychloroquine group deaths were 27 and the hydroxychloroquine plus is it through myosin best for 25 but no hydroxychloroquine.
Deaths were 18 that was statistically significant.
But here’s the interesting thing. When you look at these groups hydroxychloroquine here in this column hydroxychloroquine, is it through myosin in this column and no hydroxychloroquine? And then this p-value what this means if this P value is less than 0.05 like here then it would make sense. And this is a good way of checking it since this is hydroxychloroquine only there would be zero amount of people on his it through myosin those with hydroxychloroquine plus as it’s for my son would buy
Definition have to have as its from Ice in there and those without hydroxychloroquine might or might not have as its from my sin in there. And so the key is that these groups are statistically significantly different and that’s why the p-value is less than 0.5 in this category of Azithromycin. But if we go down and we look we can see a number of these cases where these value is less than 0.05. These groups are different when it comes to pulse oximetry. These groups are different.
Different when it comes to breaths per minute these groups are different when it comes to systolic blood pressure in certain cases and ALT and serum albumin and so forth and so forth and you can see here. These groups are very different and when you analyze this a little bit more you will start to realize quite potentially that the group that had no hydroxychloroquine. This one here actually was not as sick.
Actually as the group that got hydroxychloroquine.
And that’s exactly what they point out in this good RX blog which says that one thing to note is that people who had more severe symptoms which might partially explain the higher death rates were also more likely to get medications and that’s exactly what we see in a situation like this where you have covid-19. You have a limited number of medications in your pharmacy at the hospital and you’ve got to distribute those to those that need it the most so people who come in who are mild may not get hydroxychloroquine and azithromycin which is
We’ll say it and we’ll say it again. And again is what you need is a randomized placebo-controlled trial and is double-blinded for you to really find out whether or not this intervention Works. Those are being done and we’ll see how this goes. Also. Remember that hydroxychloroquine is being looked at as a prophylactic meeting. You start it before you get infected or maybe you start it after your infect or been exposed to prevent covid-19 from actually occurring.
So the jury is still out on hydroxychloroquine for covid-19.
Another topic that we were on pretty early in our medcram covid-19 updates was pronation or proning a patient having them lie on their bellies and we talked about that one of her early videos called how coronavirus kills and we talked about three seminal papers that were published in the New England Journal of Medicine. One of which was low tidal volumes and other one was paralysis. And then the final one was based on a French study that showed that pronating patients when they are on the ventilator can
Improve survival and also oxygenation and so there’s been a big move to prone patients while they’re awake and in some regard this might help with prevention of intubation.
Well, of course this idea has been around for some time. This was a paper that was published in 2003 where they found that there was good patient tolerance and a rapid increase in pao2 was found an intubation was avoided in all patients. No significant complications were registered. And so their conclusion was that the prone position may prove beneficial in some cases of hypoxemic respiratory failure, even in awake patients by avoiding mechanical ventilation and ventilator Associated complications. Join us at medcram.com
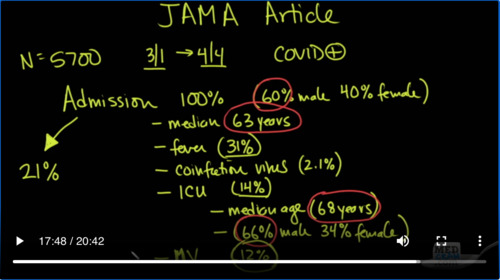
For our ventilation update the other study that I want to talk about. Is this Jama article that just came out recently and it’s important because it’s characterizing 5700 patients hospitalized with covid-19 in the New York City area. And while we’ve had studies like this before they’ve been looking at the Chinese admissions. This is the first one really that is this large in the United States. So it really is important for us to look at these numbers.
So in this situation, we had 5700 Hospital admissions from the time period of March 1st to April 4th. So who got admitted well a hundred percent got admitted to the hospital and in this situation sixty percent of them were male and of course leaving 40% female the median age was 63 years.
Interestingly how many of these patients had fever defined as a temperature of greater than a hundred point four degrees Fahrenheit or 38 degrees Celsius 31% That’s a very low number and a number that should give you pause. Remember all of these patients were covid positive patients and only 31 percent had a fever on admission how many of them had a co-infection with another virus?
Very important number to know only 2.1% how many of these patients needed to go to the Intensive Care units?
14%
now what was the median age for those that have to go to the Intensive Care Unit?
sixty-eight years
and in this group 66% were male and 34 percent were female notice that all comers to the hospital 63 was the median and then we can see what happens when we look at those going into the Intensive Care Unit. It’s those that are older also look here 60% of those being admitted to the hospital were male. Whereas those going to the Intensive Care Unit 66 were male.
How many of them need mechanical ventilation well, obviously you need to go to the Intensive Care Unit to get mechanical ventilation. So it’s going to be slightly less than 14% And in this case, it was about 12 percent of the patients that needed to be admitted to the hospital would go on to need mechanical ventilation. So here’s a real Crossroad here because of those patients that needed to be admitted to the hospital in other words in New York City between March 1st and April 4th. If you got a bit into the hospital and you were covid positive or you turned
Out to be covid positive. Your mortality rate was 21% But if you were one of the Unlucky few who 12% needed mechanical ventilation your mortality rates, if you’re going on the ventilator was a whopping eighty eight percent. So how do you go from 21 percent to eighty eight percent. It’s when you are sick enough that you need to have mechanical ventilation.
Let’s put it another way.
Let’s look at mortality.
Those aged 18 to 65 years of age and those greater than 65 years of age those who are on no vent. And those that are on the vent or had to be on the vent mortality rate for those 18 to 65. Not on the ventilator was 19.8% those greater than 65 will 26.6% on the ventilator between 18 and 65 years of age.
76.4% those on the ventilator greater than 65 years of age a whopping ninety seven point two percent mortality based on this data. Now there’s a chart here table for actually that shows age intervals and those that died and those that were discharged alive based on the decade of life. Now remember these are those patients that required hospitalization as it.
Turns out we think that that’s about 20% of all of the people who come down with the illness on average will need to go to the hospital these represent of those 20% what percents died and which ones are discharged alive.
There’s also some interesting data in the supplement where they look at those that were on Ace arbs or not on either of those two those that were discharged and those that died and really it’s very difficult to make any kind of call on whether or not they are bees or ACE inhibitors are protective or not. They make that consideration themselves in the discussion. They say however this case series design cannot address the complexity of this question and the results are unadjusted.
Unknown confounders including age sex race ethnicity socioeconomic status indicators and comorbidities such as diabetes chronic kidney disease and heart failure.
Nevertheless this study is very valuable in telling us about what are the outcomes to be expected in people who are admitted to the hospital. Now, I think an additional study should really be done on the west coast because there’s been a number of claims made that the viral strain on the east coast is substantially different than the viral strain on the west coast. It’s unclear whether or not this is the case and I think what we really ought to see is a similar paper and a patient series it.
Emitted on the west coast and see whether or not there is a substantial difference or not. Thanks for joining us.



Add comment