Dr. Seheult’s Daily Regimen; Vitamin D, C, Zinc, Quercetin, Sleep, NAC (Lecture 59)
Welcome to another MEDCRAM COVID-19 update.
The USA is still the number one in terms of new deaths reported today daily new cases in the United States show a slow decline, saying with daily deaths in the United States.
In Canada, it seems as though the daily cases are slowly trending up. Whereas the daily death seemed to be peaking at least at this point, but more time will tell. In the United Kingdom, the new daily cases are stable, but it appears as though the deaths on a daily basis seem to be attenuating somewhat in the United Kingdom.
Interesting in Australia, the daily new cases have really dropped off significantly. And it will be nice to say that. The number of daily deaths has also done that but honestly the numbers in terms of the daily deaths were pretty low to begin with a peak being a narrow 8, not to say that that’s insignificant, but it certainly is much less than compared to the United States, for instance. The number of active cases are also in decline in Australia, and that’s interesting to note because Australia is getting into the winter period here very shortly. And so it’ll be interesting to see whether or not there is a recurrence as many people have said is possible for this SARS CoV-2 virus to make a reappearance in the wintertime.
So we’ve been doing a lot of updates and we’ve been going on now for about a couple of months here on COVID-19. And I thought we would do a review and a quick thing to make it practical. And so the question is what am I doing for me, And why? and what am I doing for my patients, and why? As some of you know, I’m a pulmonary and critical care internist. I’m also a sleep specialist and I’ve been seeing patients with COVID-19 now for at least a month, I haven’t had any fevers. I haven’t had any cough, and I had a lot of questions out there about what it is that we should be doing. So I thought I’d go over what my regimen is and why I do it and go from there and I think in the next video we’ll talk about what I’m doing for my patients and why I’m doing that. Okay, let’s talk about vitamin C. Just realize that any talk that I give on vitamin C is going to be woefully underwhelming, because there is so much good information out there about vitamin C particularly in lung diseases such as ARDS and septic shock and we’ve talked before on MEDCRAM about vitamin C and its use in septic shock. Well, there’s a study here that shows that vitamin C can shorten the length of stay in the Intensive Care Unit in general. And this was a meta analysis that was done back in 2019. There’s also a really good summary on Healthline that ask the question can vitamin C protect you from COVID-19. And of course, we don’t have any evidence particularly for COVID-19 on just about anything at this point, but it does go through the data and it actually has very good resources about vitamin C and effects and what kind of research is out there, depending on the endpoint that you’re interested in. The bottom line that they come up with–they say that there’s no proof that oral vitamin C supplements will help treat or prevent COVID-19. Of course, there’s plenty of information that shows that IV vitamin C can help potentially in septic shock that was start to Marek’s group out of Eastern Virginia. And also there is another study called CITRIS ALI, which shows that vitamin C May reduce mortality in patients with a RDS I say may because mortality was a secondary endpoint in that study and by convention, they generally don’t allow you to claim something that was a secondary endpoint now for the less do I take vitamin C. Yes if I can get it in the stores I take a supplement, but I’ll also take a bowl of fresh fruit in the morning, which has lots of vitamin C and is probably more bioavailable, but you can get a lot of vitamin C from supplemental forms. I’ll talk in another video coming up about intravenous vitamin C in patients for COVID-19 in the Intensive Care Unit. That’s a big topic. We’ve covered it already for septic shock, but we’ll tackle it again.
What about vitamin D?
Well, there was this paper that was published in 2017 over 11,000 subjects in a meta-analysis of those who are on vitamin D supplementation and ask the question whether or not it could prevent acute respiratory tract infections, and the answer was yes.
Here’s a list of all the studies that they did the meta-analysis on. And you can see that the majority of these boxes were to the left of the solid Blue Line running down the middle here at one showing you that overall had a statistically significant P value of 0.001, meaning that there was definitely a benefit taking vitamin D supplementation. But there were a couple of interesting side points to this. What they found was that if you treat 33 people with vitamin D supplementation, you could prevent one acute respiratory tract infection. That sounds like a lot of people that that’s actually not that bad in terms of pharmacology generally speaking treating somebody with Aspirin for a myocardial infarction is around the same number. They also found that it was better getting a daily or weekly vitamin D dose rather than a bolus dose when you were sick and that those with vitamin D deficiency, which let me tell you is not uncommon. The number needed to treat was only for that is an astoundingly low number needed to treat, which, of course, means that the effect is very powerful.
There was another study that was published from Trinity College Dublin looking at Irish people and whether or not vitamin D could help them. This is brand new data just published a few weeks ago. And this is known as ‘the TILDA’ or ‘the Irish longitudinal study on Aging’. What they found in this study was that in some people vitamin D supplementation could reduce the incidence of chest infections by 50% That’s a 5-0. Now, of course in Ireland they have a lot of overcast days. I live in sunny Southern California, but I can tell you that a number of patients have vitamin D deficiency and it’s simply because we’re inside all the time. We don’t get the benefit of being in the sun. So it really doesn’t matter where in the world you are. If you’re inside the whole time, you’re not going to get enough sun exposure to get vitamin D.
So do I take Vitamin D supplements? You bet. and I actually take about 2,500 international units a day. That’s about sixty-two point five micrograms a day. You may be wondering what dose is right for you and it’s complex. It’s so it depends on your age and a number of other factors. So my recommendation is to talk to your healthcare provider and you actually may need to be tested and put on supplementation and retested for some of you.
I also take care certain Quercetin and I have to say the reason why I take Quercetin is because of the early studies on hydroxychloroquine now hydroxychloroquine as we’ve talked about before has a number of mechanisms that might inhibit the virus SARS-CoV2 from replicating in the cell. One of those mechanisms is that it changes the pH of the endosomes that are needed for the virus to come into the cell and that can prevent entry of the virus into the cell.
Another mechanism is through a zinc Ionaform hydroxychloroquine is a zinc ionaform and as such, when zinc comes into the cell that can shut down the replicase enzyme that the tsar’s cup of two virus needs to replicate. Well, as it turns out Quercetin is also a zinc Ionaform Quercetin is found naturally in onions Capers and other food products. You can get it over the counter. I take about 500 milligrams twice a day and just as a side note Quercetin is being studied by a Chinese and Canadian researcher in China to see if it makes any difference with respect to COVID-19.
Another supplement that I take is n-acetylcysteine, otherwise known as NAC and this is another over-the-counter medication. And why do I do that? Well, it’s because of this 1997 paper titled ‘attenuation of influenza like symptomatology and Improvement of cell-mediated immunity with long-term and acetyl system treatment’. Basically, what it showed was when NAC was given 600 milligrams twice daily for six months while it didn’t reduce the chances of getting the influenza virus. It significantly attenuated the severity of the influenza like illness, especially in elderly and high-risk individuals and the difference was astounding 79 percent of people in the placebo group had symptoms of the influenza virus, whereas only 25% of the virus infecting subjects under NAC treatment developed a symptomatic form of the virus. And basically, what n-acetyl cysteine is doing is it’s helping out the liver in terms of reducing glutathione reducing is the opposite of oxidizing, so it’s an antioxidant essentially. And it helps the liver in terms of getting rid of toxins. By the way, this is also the same medication that we give in patients who overdose on Tylenol again helping out the liver. So I take 600 milligrams two times a day.
Okay, so I also take a zinc supplement. And if you want to know more about why well, we just talked about the replicase enzyme from SARS Cove to but you could also go back and look at MEDCRAM updates numbers 32 and 34. So I only take about 50 milligrams of zinc during these periods of time where I think I might be exposed to the virus. You have to be careful taking 50 milligrams of zinc a day because that is above the recommended daily dose of 40 milligrams and there is some concern that taking doses higher than 40 milligrams daily might decrease how much copper the body can absorb. So it’s not something I would do on a regular basis. The other thing that I try to do on a regular basis is sleep. That may sound crazy but we actually have good data that sleep is really important. And if you want to know more information about sleep I encourage you to go to our MEDCRAM updates numbers 16 17 and 45. And the dose of sleep that I like to get here is seven to eight hours per night.
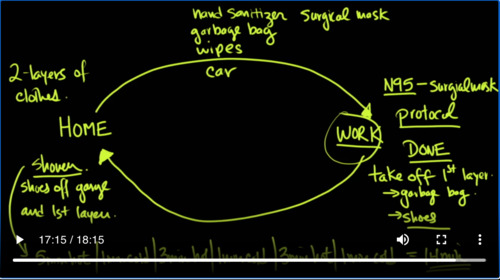
Now I’m going to tell you about my routine when I actually go to work, because I see patients with COVID-19 almost on a daily basis, but I’ll tell you the nurses and the respiratory therapists are exposed to those patients far more than I am and so part of the reason why I’m doing this is to make sure that they are also protected. I don’t want to see any of the nurses or the people that I work with get sick with this virus. So the first thing is let’s talk about going to work and of course I go to work in my car and the things that you should have in your car. Number one is you should have a hand sanitizer. You should have a garbage bag. You should have disinfectant wipes. You should also have a surgical mask. Right now in California, We are required to have a mask if we get out of the car and walk around in a public area and that would mean going into a hospital. So when I get up and go to my car to drive to work, I have two layers of clothes on and that’s usually an undershirt pants and then I put over that my scrubs so I jump in my car and I drive to work. When I’m at work, I typically put on an n95 mask and I cover it with a surgical mask that n95 mask is mine for the rest of the day and in some of the hospitals that I work in they will recycle that mask and give me a new n95 mask or a recycled n95 mask the next day but what that surgical allows me to do is to protect that n95 mask which is more valuable and I can take off the surgical mask when I come out of a patient’s room because the virus may be airborne and they settle on my surgical mask and that way I don’t have to worry about contaminating my n95 mask. The other thing that you need to do is make sure you follow your protocol whatever it happens to be at your work in terms of entering and exiting. It’s almost a piece of cake putting on the personal protective equipment. Which really difficult is remembering in which order to take it off and making sure that you don’t contaminate yourself and the rule of thumb there generally speaking is no matter what you do. You always end it with a hand sanitizer. So generally speaking what I was doing after I had gone in to see a patient and I would go into the anti-room or the room right before you come out is you would take off the shoe covers and then hand sanitized and take off the cap that is on your head and then hand sanitizer and then you would take off the surgical mask on the n95 mask and then hand sanitizer. Then you take off your gown and then you would hand sanitizer in some order to that degree before eventually you would come out only with the goggles protecting your eyes and the n95 Masks then wash your hands with soap thoroughly before touching your face, of course and try not to touch your face at all. Sometimes we would even use Peppers as they’re called to make sure that you have a positive pressure around your face to make sure that you don’t breathe in the virus.
And these are especially handy if you’re doing procedures that could cause aerosolization of the virus. Then when you’re done at the end of the day, it’s time to come back home some of the staff that I know would sometimes take showers and they would it bring an extra change of clothes. They would have showers there at the hospital. I decided not to do that. But instead when I got to my car I also didn’t want to contaminate my car and so because I had another layer of clothing underneath I would take off the first layer at work. Then, I would put that into the garbage bag that was handy in the car. Then I would use hand sanitizer. I would use the wipes on my shoes because you know that there’s got to be a virus on the ground. So I would wipe my shoes. I would put all of the clothes into a garbage bag. I will put that into the trunk. I would hand sanitize. I would hand sanitize the steering wheel and at that point I would then drive home.
If you need to get gas, make sure you have an appropriate first layer of clothing. So you could actually go into the gas station. Then when you got home I would make sure to take my shoes off in the garage as well as just about anything else that I could in the garage and depending on who you talk to nurses doctors. They’ll tell you whether or not they’re completely Stark naked in the garage or got underwear on usually those clothes would go into the garbage bag as well. And those clothes would go directly into the washing machine and go on hot. Whereas I would go directly upstairs into the shower before going anywhere else.
But it’s not just any shower that I would take. It was five minutes of hot as hot as you could take and then one minute of really cold as cold as you could take and then three minutes of as hot as you could take and then one minute as cold as you can take and then three minutes as hot as you could take and then finally ending up with one minute as cold as you can take.And the total there would be 14 minutes of shower. So you’re probably wondering “well, why would I do that?” Well, if I was going to be infected with the virus, it would have been here at work. And by the time I get home, we’re within 12 hours because each shift is about 12 hours. So if there’s any appointed time that I want to have a good immune system specifically a good innate immune system. That’s the time. I would have it. What does this have to do with a good immune system? We’ve talked about this before especially in MEDCRAM updates 46 and 47. One of the things that we talked about in update 47 was this thing called the contrast shower where you do five minutes of hot one minute cold three minutes hot one minute cold three minutes hot woman at cold and that’s exactly what I’m doing. Now. Remember we have no randomized controlled trials at all with COVID-19. We don’t know to the level of evidence that were normally comfortable with what it is that works with COVID-19 and a lot of the stuff that I’m showing here. I don’t have absolute proof that it works. But a lot of the stuff that we’re doing here really doesn’t have a lot of risk.
In an upcoming video, I’m going to show you some of the stuff that we’re doing for patients and what I’m doing for patients. And we’ll review that data and look at the evidence for it. But in the meantime, I wanted to show you what at least I was doing to protect myself and also my family, you know, one of the things that I really enjoy about MEDCRAM is the response that I get from you the viewers. And sometimes I feel like I learn more from the comments that I get after a video then the research that I put into the video. We read all of the comments. We just don’t have time to answer all the comments or even all the emails that we get, but we know that there’s some really good ideas out there and to harness that we’ve created some communities. We’ve currently set up COVID-19 community and the MEDCRAM in general community and it’s really open to anyone. It’s for questions ideas evidence-based information, and all you need is just to sign up with an account and start posting. I think the best result happens when there’s a cross-pollination of ideas. Thanks for joining us.
Questions that may be asked:
- What is the possible mechanism of vitamin C and D in combating COVID-19?
- What kind of routine precautions that are recommended by the speaker for healthcare providers working at hospitals fighting COVID-19?
- What do scientist think about the prevalence of the pandemic in Australia will be, and why?
- I’m rather interested in the basic principles and methods of meta-analysis after listening to this lecture, can you tell us more about it?



Add comment