The ACE2 Receptor – The Doorway to COVID-19 (ACE Inhibitors & ARBs) (Lecture 37)
Welcome to another MedCram covid-19 update. You can see the numbers here. They are starting to exceed that of mainland China when we look globally. What I want to get to today is something that a lot of you have commented on, and that is the receptor for the SARS-cov-2 virus that causes covid-19.
欢迎来到MedCram covid-19的另一个更新。您可以在此处看到数字。当我们放眼全球时,它们已开始超过中国大陆。我今天要说的是很多人都在评论的东西,那是引起covid-19的SARS-cov-2病毒的受体。
That is the ACE2 receptor. The ACE2 receptor is how the virus gets into the cell. It’s the doorway and it’s more than just the doorway. Today, we’re going to be talking about exactly what the ACE2 receptor is, and what it’s involved in, and why that matters.
那就是ACE2受体。 ACE2受体是病毒进入细胞的方式。ACE2受体不仅仅是病毒进入细胞的通道。今天,我们将要确切讨论ACE2受体是什么,它涉及什么以及为什么重要。
I’ve been wanting to do this for a long time. But the more I looked into it, the more complicated and interesting at the same time that it was. So I want to do the research first and then tell you where we are right now. This has reached ahead because there are a number of people out there that are actually taking different sides on this issue of the receptor. So what it boils down to basically as we’ve talked before outside of the cell, on the surface of the cell, there is a receptor for the SARS-COV-2 virus, which is the thing that causes covid-19, which is the coronavirus.
我一直想这样做。但是,我研究的越多,同时它就越复杂和有趣。因此,我想先进行研究,然后再告诉您我们现在的位置。之所以能做到这一点,是因为实际上有很多人在受体问题上有不同的立场。所以基本上可以归结为我们之前在细胞外部所说的那样,在细胞表面,有一个SARS-COV-2病毒的受体,它是导致covid-19冠状病毒的原因。
Here we have the virus, and it’s got these projections that make it look like rays of the sun. That’s why it’s called the coronavirus. This is SARS-COV-2; this is 2019 coronavirus. Here is the S protein that we’ve talked about, and the receptor for this is on the surface of the cell, specifically cells that are found in the lung, the type-2 pneumocytes it’s known as, and also in the GI tract.
在这里,我们有病毒,而且有这些预测使它看起来像太阳的光芒。这就是为什么它被称为冠状病毒。这是SARS-COV-2;这是2019年的冠状病毒。这是我们已经讨论过的S蛋白,它的受体在细胞表面,特别是在肺部,已知的2型肺细胞以及胃肠道中发现的细胞。
This receptor is known as ACE2, and that’s really important for you to understand ACE2. This is where the S protein docks, and then there’s another protein called a serine protease, which is also here in the membrane, which helps to internalize this virus into the cell, and it allows the messenger RNA, which is in here, to come in and infect the cell. The key here though is this protein, that is on the side of the cell, is ACE2, and it’s exactly the same protein that was the receptor for the SARS-cov virus that was back in 2002.
该受体称为ACE2,这对于您了解ACE2确实很重要。这是S蛋白停靠的地方,然后还有另一种称为丝氨酸蛋白酶的蛋白,它也在膜中,这有助于将该病毒内化到细胞中,并允许其中的信使RNA进入并感染细胞。然而,关键是这种蛋白质位于细胞侧面,是ACE2。它与2002年SARS-cov病毒的受体完全相同。
So the question is why is this such a problem? Well, there is some animal data that angiotensin receptor blockers, which is a very common type of high blood pressure medication and ACE inhibitors, which is another common type of blood pressure medication, can increase the concentration of these ACE2 receptors on the surface of the cell.
那么问题是:为什么这是一个问题?好吧,有一些动物数据表明,血管紧张素受体阻滞剂是一种非常常见的高血压药物,而ACE抑制剂是另一种常见的高血压药物,可以增加这些ACE-2受体在细胞表面的浓度。
How do you know if you’re on an ARB or an ACE inhibitor? Typically ARBs end in ‘TAN’, so you might see this as losartan, or irbesartan or candesartan. These are all TANs. They are angiotensin receptor blockers. We’re going to talk more about what they do.
您怎么知道您使用的是ARB还是ACE抑制剂?通常,ARB以’TAN’结尾,因此您可能会看到这是氯沙坦,厄贝沙坦或坎地沙坦。这些都是TAN。它们是血管紧张素受体阻滞剂。我们将更多地讨论他们的工作。
If it’s true that they could increase ACE2 levels, it seems like it will be common sense that if you have more ACE2 receptors on the surface of your cell, now you’ve got more entry points for the virus to infect your cell. ACE inhibitors, they typically end in PRIL, so captopril, enalapril, and the list goes on. Those can also increase potentially your ACE2 receptors.
如果它们确实可以增加ACE2的水平,这似乎是常识,如果您的细胞表面有更多的ACE2受体,那么现在病毒有更多的细胞感染入口点了。 ACE抑制剂通常以PRIL结尾,因此卡托普利,依那普利依此类推。这些也可能会增加您的ACE2受体。
What do we do with patients who are on ARBs and ACE inhibitors? Well, it seems as though people have higher mortality who have a history of hypertension. So this has led to a number of articles and a lot of social media to talk about “should we get off of our medications that we’re taking for high blood pressure?”
对于使用ARB和ACE抑制剂的患者,我们该怎么办?好吧,似乎有高血压病史的人死亡率更高。因此,这导致了许多文章和许多社交媒体谈论“我们应该放弃高血压服用的药物吗?”
Here is an article that was sent to the Lancet. It was published on March 11th, 2020. The question is “Are patients with hypertension and diabetes mellitus at risk for covid-19 infection?” They talked about the incidence of cardiovascular diseases. They talked about the SARS-COV virus and SARS-cove-2, and the ACE-2 protein which is the receptor for this, and they talked about how ACE inhibitors and ARBs increase ACE expression. The increased expression of ACE2 would facilitate infection with covid-19. They therefore hypothesize that diabetes and hypertension treatment with ACE2 stimulating drugs increases the risk of developing severe and fatal covid-19.
这是发送给柳叶刀的文章。它于2020年3月11日发布。问题是“高血压和糖尿病患者是否有可能发生covid-19感染的危险?”他们谈论了心血管疾病的发病率。他们谈论了SARS-COV病毒和SARS-cov-2,以及作为其受体的ACE-2蛋白,并谈论了ACE抑制剂和ARB如何增加ACE表达。ACE2表达的增加将促进covid-19的感染。因此,他们假设使用ACE2刺激药物治疗糖尿病和高血压会增加发生严重和致命的covid-19的风险。
Now, this is only a hypothesis. They say if this hypothesis were to be confirmed, it would lead to a conflict regarding the treatment because ACE2 reduces inflammation. It has been suggested as a potential new therapy for inflammatory lung diseases, cancer, diabetes and hypertension, a further aspect that should be investigated is the genetic predisposition for an increased risk of SARS-cov-2 infection, which might have to do with ACE2 polymorphisms, they say.
现在,这只是一个假设。他们说,如果这一假设得到证实,将因ACE-2减轻炎症而导致治疗冲突。有人建议将其作为治疗炎症性肺疾病,癌症,糖尿病和高血压的潜在新疗法,应进一步研究的是遗传易感性,其可能导致SARS-cov-2感染的风险增加,这可能有关AC2多态性。
Finally, they say they suggest that patients with cardiac disease, hypertension or diabetes, who are treated with ACE2-increasing drugs, are at higher risk for severe covid-19 infection, and therefore they should be monitored for ACE2 modulating actions such as ACE inhibitors or ARBs. They did not find any evidence to suggest that antihypertensive calcium channel blockers increase ACE2 expression or activity. Therefore these could be suitable alternative treatments in these patients.
最后,他们说,建议使用增加ACE2的药物治疗的心脏病,高血压或糖尿病患者,发生严重covid-19感染的风险更高,因此应监测ACE2调节作用,例如ACE抑制剂或ARB。因没有发现任何证据表明降压钙通道阻滞剂会增加ACE2的表达或活性。这些可能是这些患者的合适替代疗法。
Here we have an article, a correspondence to a very major journal, which is raising an alarm on millions of patients who are on these medications and saying that they hypothesize that the patients could be at risk. Obviously, this has raised quite a stir, and the question is “is there any actual truth to this?”
在这里,我们有一篇文章,与某本非常重要的期刊相对应,正在对数百万使用这些药物的患者发出警报,并说他们假设患者可能处于危险之中。显然,这引起了极大的轰动,问题是“这是否有任何真实的事实?”
So let’s look and see what the response has been. Here is the response from the European Society of Cardiology. They say because of social media related amplification, these patients taking their high blood pressure medications have become increasingly concerned, and in some cases stopped taking their ACE or ARB medications.
因此,让我们看一下响应是什么。这是欧洲心脏病学会的回应。他们说,由于社交媒体相关的放大作用,这些服用高血压药物的患者越来越受到关注,在某些情况下停止服用ACE或ARB药物。
This is what the official response from the European Society for Cardiology: ” the speculation about the safety of ACE inhibitors and ARB treatment in relation to covid-19 does not have a sound scientific basis or evidence to support it. Indeed, there is evidence from studies in animals suggesting that these medications might be rather protective again serious lung complications in patients with covid-19 infection. To date, there is no data in humans.
这是欧洲心脏病学会的官方回应:“关于与covid-19相关的ACE抑制剂和ARB治疗的安全性的推测没有可靠的科学依据或证据。实际上,对动物的研究表明,这些药物可能对患有covid-19感染的患者再次起到保护肺部严重并发症的作用,迄今为止,尚无人类数据。
The Council on Hypertension for the European Society of Cardiology wishes to highlight the lack of any evidence supporting harmful effect of ACE inhibitors and ARB in the context of the pandemic covid-19 outbreak. They strongly recommend that physicians and patients should continue treatment with their usual antihypertensive therapy because there is no clinical or scientific evidence to suggest that treatment with ACE inhibitors or ARBs should be discontinued because of the covid-19 infection.”
欧洲心脏病学会高血压委员会希望强调指出,在covid-19背景下,缺乏任何证据支持ACEI和ARB的有害作用。他们强烈建议医师和患者应继续采用常规的降压疗法进行治疗,因为没有临床或科学证据表明由于covid-19感染而应终止使用ACE抑制剂或ARB的治疗。”
So what is it? Which one of these is correct? To delve into the intricacies of that, we’re going to go into some molecular biology. At some point, we’ll get a little complicated, but not too. So bear with me as we go through a detailed instruction on exactly what is going on with the SARS-CoV-2 virus and the renin-angiotensin system.
那是什么?以下哪一项是正确的?为了探究其复杂性,我们将研究分子生物学。在某些时候,我们会变得有些复杂,但事实并非如此。因此,请跟随我详细了解SARS-CoV-2病毒和肾素-血管紧张素系统的确切过程。
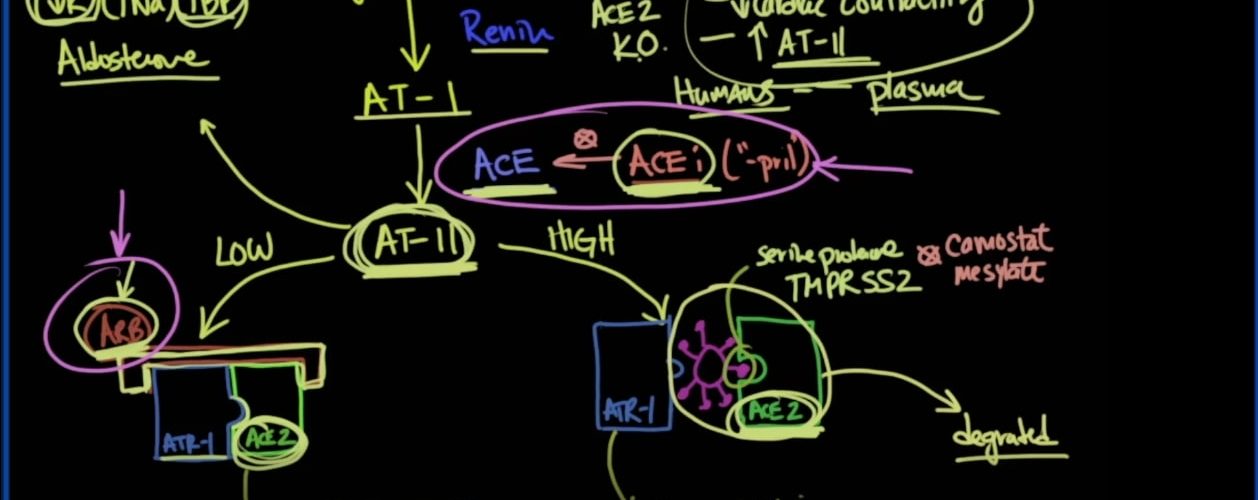
To understand this, you first start off with a hormone called angiotensinogen, and that is converted into angiotensin I, which will abbreviate AT-1, and that is done through an enzyme called renin that is produced by the kidney. Angiotensin I is then converted into Angiotensin II, and that is done in the lung by an enzyme called ACE.
要了解这一点,首先要从一种叫做血管紧张素原的激素开始,然后将其转化为血管紧张素I,后者将缩写为AT-1,这是通过肾脏产生的一种称为肾素的酶来完成的。然后将血管紧张素I转化为血管紧张素II,并通过称为ACE的酶在肺中完成。
Now ACE is in the lung; it does convert angiotensin I to Angiotensin II, and we can inhibit ACE by giving someone an ACE inhibitor, and these are the medication that end in PRILs, so captopril and lisinopril, etc.
现在ACE在肺中。它确实将血管紧张素I转换为血管紧张素II,我们可以通过给予ACE抑制剂来抑制ACE,而这些都是以PRILs终止的药物,例如卡托普利和赖诺普利等。
Angiotensin II is a powerful vasoconstrictor. It also stimulates the adrenal gland to make aldosterone, which has the action of lowering potassium and increasing sodium concentration, therefore increasing blood pressure.
血管紧张素II是强大的血管收缩剂。它还刺激肾上腺生成醛固酮,该醛固酮的作用是降低钾和增加钠的浓度,从而增加血压。
Angiotensin II is a major dividing point because there are two types of states that one can have in the body. So we’ll call this the low state, and we’ll call this the high state. On the cell membrane is a component of proteins that are sitting out on top of the cell membrane, and one of those is ACE2.
血管紧张素II是主要的区分点,因为人体中有两种种状态。因此,我们将这个称为低状态,将那个称为高状态。在细胞膜上的是位于细胞膜顶部的蛋白质的一种成分,其中之一就是ACE2。
When there is not a lot of Angiotensin II around, it is proposed Angiotensin receptor 1 ( ATR1) sits in the catalytic site of ACE2. Now as it turns out, Angiotensin II will be converted by ACE2 into Angiotensin 1, 7. It’s very important for you to understand Angiotensin 1,7 because Angiotensin 1,7 causes vasodilation and decreases inflammation. That’s a good thing.
当周围没有大量血管紧张素II时,建议血管紧张素受体1(ATR1)位于ACE2的催化位点。现在事实证明,血管紧张素II将由ACE2转换为血管紧张素1、7。了解血管紧张素1,7对您非常重要,因为血管紧张素1,7会引起血管舒张并减少炎症。这是好事。
It’s also possible that you could put and have an Angiotensin receptor blocker that would block this, and that is an ARB. So we’ve talked about Angiotensin receptor blockers, and we’ve talked about ACE inhibitors.
您也可能会放一个血管紧张素受体阻滞剂来阻止它,那就是ARB。因此,我们讨论了血管紧张素受体阻滞剂,也讨论了ACE抑制剂。
If you have high Angiotensin II, this is the situation that you get. You still have ACE2, but the high levels of Angiotensin II cause the Angiotensin receptor to come off of ACE2. When that happens, when Angiotensin II interacts with Angiotensin receptor 1, the result of that is vasoconstriction, increased blood pressure, increased vascular permeability, pulmonary edema, and presumably ARDS.
如果您的血管紧张素II高,就会出现这种情况。您仍然拥有ACE2,但是高的血管紧张素II会导致血管紧张素受体从ACE2脱落。发生这种情况时,当血管紧张素II与血管紧张素受体1相互作用时,其结果是血管收缩,血压升高,血管通透性增加,肺水肿,可能是ARDS。
Furthermore, when there’s high Angiotensin II, the hypothesis is that this opening in ACE2 allows for the coronavirus with its S protein to bind to ACE2. This binding here also requires something called a serine protease, known as TMPRSS2. Now that can be inhibited with something called camostat mesylate, and that is undergoing trials right now. Interestingly, when you have high levels of AT-II, this entire complex gets degraded into lysosomes.
此外,当血管紧张素II高时,推论是ACE2中的此开口允许带S蛋白的冠状病毒与ACE2结合。这种结合在这里也需要一种叫做丝氨酸蛋白酶的东西,称为TMPRSS2。现在,可以用一种叫做camostat甲磺酸盐的东西抑制这种现象,并且目前正在试验中。有趣的是,当您具有高水平的AT-II时,整个复合物会降解为溶酶体。
So let’s review quickly. We’ve got angiotensinogen being converted to Angiotensin I by renin. Angiotensin I is converted to Angiotensin II by an ACE enzyme. ACE inhibitors can prevent that from happening. If you have too much of angiotensin II, then what can happen is that Angiotensin receptor blocker dissociates with ACE2, and it gets activated to cause vasoconstriction, increase blood pressure, permeability, pulmonary edema, and ARDS. That’s exactly what we don’t like to see in these situations in viral pneumonia.
让我们快速回顾一下。我们已经将血管紧张素原由肾素转化为血管紧张素I。血管紧张素I通过ACE酶转化为血管紧张素II。 ACE抑制剂可以防止这种情况的发生。如果您的血管紧张素II过多,则可能发生的情况是血管紧张素受体阻滞剂与ACE2分离,并被激活引起血管收缩,增加血压,通透性,肺水肿和ARDS。这就是我们不希望在病毒性肺炎的这些情况下看到的。
However, if there are low levels of angiotensin II, then what we see is that it gets metabolized by ACE2, and that gets converted into a vasodilator called Angiotensin 1,7. Also, it looks as though ARBs, or Angiotensin receptor blockers, can somehow keep this complex together and keep that catalytic site blocked by the resident ATR Angiotensin receptor, and that can happen with Angiotensin receptor blockers. If angiotensin II is high, however, this dissociation occurs, allowing the virus to potentially bind according to the hypothesis, and that causes degradation.
但是,如果血管紧张素II含量低,那么我们看到的是血管紧张素II被ACE2代谢,然后转化为血管扩张剂,称为血管紧张素1,7。而且,似乎ARBs或血管紧张素受体阻滞剂可以某种方式使该复合物保持在一起,并使催化位点被驻留的ATR血管紧张素受体阻滞,而血管紧张素受体阻滞剂可能会发生这种情况。但是,如果血管紧张素II高,则会发生这种解离,从而使病毒可能根据推论进行结合,从而导致降解。
So what do we see in people who have no ACE? If we take away all of their ACE2, as we’re showing here, what happens? Well, they’ve actually done this in mice. They’re able to breed mice where they delete the gene responsible for making ACE2.
那么,在没有ACE的人中我们会看到什么呢?如果我们如此处所示将所有的ACE2拿走,会发生什么?好吧,他们实际上已经在老鼠身上做到了。他们能够在小鼠中繁殖出删除负责制造ACE2的基因的小鼠。
They’re called Knockouts. Double Knockouts mean they take it both on the mother’s side and the father’s side, so when the mouse is born, it has no ACE2 whatsoever. They’ve shown that these mice have a resistance to being infected with the virus because there’s no receptor.
他们被称为敲除。 双敲除(Double Knockouts)意味着他们可以同时在母亲和父亲这边敲除它,因此,当老鼠出生时,它就没有ACE2。他们已经证明这些老鼠对这种病毒没有抵抗力,因为它们没有受体。
But at the same time, what they see in these knockout mice is that they have worse outcomes in viral pneumonia. They have decreased cardiac contractility, and they have increased levels of Angiotensin II, which makes sense because it’s ACE2 which breaks down Angiotensin II when there is a low amount of it.
但与此同时,他们在这些基因敲除小鼠中看到的是它们在病毒性肺炎中病得更重。他们的心脏收缩力下降,血管紧张素II水平升高,这是有道理的,因为当血管紧张素II含量低时,它是由ACE2分解的。
So these are in what we call ACE2-knockout mice, and these are exactly the things that we’re seeing in patients who are infected with the coronavirus. What they saw in a mouse model of SARS-CoV from 2002 was that there were decreased levels of ACE2 in these viral models, and they had normal ACE levels, but there were less ACE2 levels. They also saw increased levels of Angiotensin II, and when they gave these mouse models ARB, and they gave them ACE inhibitors, this actually improved the outcomes. I’ll show you the links to those studies in the description below.
这些就是我们所说的ACE2敲除小鼠,而这正是我们在感染冠状病毒的患者中看到的东西。他们从2002年的SARS-CoV小鼠模型中看到的是,这些病毒模型中ACE2的水平降低,并且它们的ACE水平正常,但ACE2水平较低。他们还发现了血管紧张素II的水平升高,当给这些小鼠模型ARB和ACE抑制剂时,这实际上改善了结果。我将在下面的说明中向您显示这些研究的链接.
In a respiratory syncytial virus case, they actually took recombinant ACE2 and gave it to these mouse models, and they found that it improved outcomes. So you can see according to the animal hypothesis, that if you added an ACE inhibitor, it would block this ACE enzyme, making sure that this angiotensin II was on the low side.
在呼吸道合胞病毒的情况下,他们实际上服用了重组ACE2并将其用于这些小鼠模型,结果发现它们可以改善结局。因此,根据动物假说,您可以看到,如果添加ACE抑制剂,它将阻止该ACE酶,并确保该血管紧张素II处于低位。
But what we may be seeing is that these Angiotensin levels are actually on the high side, and you would predict that if Angiotensin II levels were on the high side, you would expect there would be aldosterone, and low potassium, and high blood pressure. That’s exactly what they saw in very very sick covid-19 patients is that they were hypokalemic, which means low potassium. The most critical of these had higher blood pressure before they crashed.
但是我们可能会看到,这些血管紧张素水平实际上偏高,您可以预测,如果血管紧张素II水平偏高,则您会预期会有醛固酮,低钾和高血压。他们在非常重病的covid-19患者中看到的正是他们的低钾血症,这意味着低钾。其中最严重的是在死亡前血压升高。
You can also see here how keeping somebody on an Angiotensin receptor blocker, according to this hypothesis, may improve this kind of a situation, leading to vasodilation and anti-inflammation.
您还可以在这里看到,根据这个假设,如何让某人继续使用血管紧张素受体阻滞剂可以改善这种情况,从而导致血管舒张和消炎。
I want to emphasize that while we have good data in mice, when we look at humans, we don’t see these kinds of things happening, at least in the plasma in free-floating ACE. We don’t know what’s going on at the tissue level. So it still may be happening. So the thing I want to stress here is that this is all a hypothesis based on piecing together studies over the last 20 years that they feel that this may be what’s happening. If you’re interested in this kind of research, I’m going to put a bunch of links in the description below that link to the papers that talk about this.
我想强调的是,尽管我们在小鼠中拥有良好的数据,但是当我们观察人类时,至少在自由漂浮的ACE血浆中,我们看不到这种事情的发生。我们不知道组织水平上发生了什么。因此它可能仍在发生。因此,我在这里要强调的是,所有假设都是基于过去20年将研究结合在一起而得出的,他们认为这可能正在发生。如果您对这种研究感兴趣,我将在下面的描述中添加很多链接,这些链接指向讨论此问题的论文。
But suffice to say that at this point to go out and say that we should be stopping people on their ACE inhibitors and stopping people on their ARBs, in my humble expert opinion, as much as you want to consider me an expert on this, I would say that the jury is out, and I believe I would come down on the side of the statement from the European Society for Cardiology and saying we really don’t know at this point, and we have some animal studies which actually show that they may be protective in this case.
但是,我要谦虚地说,在这一点上说我们应该停止使用ACE抑制剂的人,停止使用ARB的人,就像您想让我成为专家一样,会说陪审团已经出庭了,我相信我会拒绝欧洲心脏病学会的发言,并说我们真的不知道这一点,而且我们进行了一些动物研究,实际上表明它们在这种情况下可能是保护性的。
There’s been a number of reports on the deaths in covid-19 that their ejection fractions, or their cardiac contractility, have been fine when they come in hospital, but over a couple of days of either viral myocarditis, or because of this situation that we’re seeing here that their contractility has dropped significantly as we would expect when ACE2 levels go down.
有许多关于covid-19死亡的报道,他们的射血分数或心脏收缩力在住院时都很好,但是经过几天的病毒性心肌炎或由于这种情况,在这里,他们的收缩力已经大大下降,正如我们预期的那样,当ACE2水平下降时。
So this is something that needs to be addressed, and we don’t know exactly what is going to happen until we have those studies. The good news is, according to what I have seen in the last couple of days, there is research looking into starting patients on Angiotensin receptor blockers, or ARBs, so that was a very long explanation over something that has come up very recently.
因此,这是需要解决的问题,直到我们进行了这些研究,我们才确切知道会发生什么。好消息是,根据我最近几天所看到的,有研究正在研究使用血管紧张素受体阻滞剂(ARB)的初次患者,因此对于最近出现的情况进行了很长的解释。
I think we should continue to delve into this receptor issue, especially when it comes to talking about vaccines because ACE2 is going to play an extremely important role in the future of treatment of covid-19. Thank you for joining us.
我认为我们应该继续研究这个受体问题,尤其是在谈论疫苗时,因为ACE2在covid-19的未来治疗中将发挥极其重要的作用。感谢您加入我们。



Add comment