医院和诊所如何为COVID-19做好准备
How Hospitals & Clinics Can Prepare for COVID-19, Global Cases Surge (Lecture 38)
Welcome to another MedCram covid-19 update. Here, we see 182,000 confirmed; total death 7100; total recovered 79,000. The map is turning into basically a red blob.
欢迎来到MedCram covid-19的另一个更新。在这里,我们看到182,000已确诊;总死亡7100;总共恢复79,000。该地图基本上变成了红色斑点。
I want to go over to the WorldOmeter website and show you some interesting trends. We see here the total cases starting to accelerate once again because we’re reaching an epidemic phase outside of China. If we look here at total deaths, they are also being mirrored. If we looked at active cases, we can see here that there was a plateauing, even a dropping off as China was containing what was going on. Then outside of China here in Italy, South Korea and now United States, we’re starting to see an increasing number of those active cases.
我想转到WorldOmeter网站,向您展示一些有趣的趋势。我们在这里看到总病例数再次开始加速,因为我们正处于中国境外的流行阶段。如果我们在这里查看全部死亡人数,那么它们也正在被镜像。如果我们研究活跃的案例,我们可以看到这里处于平稳期,甚至随着中国遏制正在发生的事情而下降。然后在中国之外的意大利,韩国和现在的美国之外,我们开始看到越来越多的此类活跃病例。
But here’s something that’s very interesting. In the close cases, when we show the graph for that, we’re actually starting to see that there is an upturn here in the death rate where they’ve either gotten better or they’ve passed now. There are only two reasons that I could see for the death rate to be increasing; either number one: the virus is mutating and becoming more deadly; or number two: there is a lot less testing and the number of active cases is going up much more. So I suspect given the fact that the death rate is going up, there are a lot more cases that are just not being picked up out there because of lack of testing.
但是,这很有趣。在较近的情况下,当我们显示该图时,我们实际上开始发现死亡率有所提高,他们要么变得更好,要么就已经过去了。我能看到死亡率上升的原因只有两个;任一个:病毒正在变异并变得更加致命;或第二名:测试少了很多,有效病例的数量却增加了很多。因此,我怀疑鉴于死亡率正在上升的事实,由于缺乏测试,还有更多的病例没有被拿出来。
We can see here that in China, where there was a rip-roaring infection, of course at the beginning, the total cases per million population was 56. We’re seeing a much higher number here in Iran and Spain and even in South Korea, in Italy. We don’t have that number here, but we can see that those numbers are quite high and would probably be very large. In terms of the United States, we’re seeing very small numbers. The question is whether or not that’s because of lack of testing.
我们在这里可以看到,在中国,这里一开始就是激怒的感染,当然,每百万人口中的总病例数为56。在伊朗,西班牙甚至韩国,我们看到的病例数要高得多, 在意大利。我们这里没有那个数字,但是我们可以看到那些数字很高,可能很大。就美国而言,我们看到的数字非常少。问题是那是否是因为缺乏测试。
If we look again at the active cases list, we see here by far the most amount of active cases going on right now is in Italy, and that is the tragedy right now. What is going on in Italy? Because there are so many active cases happening so quickly that their healthcare system is being overwhelmed.
如果我们再次查看活跃病例列表,那么我们在这里看到的是目前发生的最多的活跃病例是在意大利,这就是现在的悲剧。意大利发生了什么事?因为有这么多活跃的病例发生得如此之快,以至于他们的医疗系统不堪重负。
I want to go back to this notion of ‘flattening the curve’. I think there are some other things that we need to talk about. So if this represents the number of patients over time, and this dashed line represents the capacity of the health system, then clearly what is going on right now in Italy is something that looks like this, and we can only hope that it starts to come down quickly.
我想回到“扁平化曲线”的概念。我认为我们还有其他事情要谈。因此,如果这表示一段时间内的患者人数,而该虚线表示卫生系统的能力,那么显然意大利现在正在发生的事情看起来像这样,我们只能希望它开始出现快速下降。
What we are trying to do here in the United States is slow down the rise of this so that we’re able to take care of these patients that are coming into the hospital. So the question here is “is this going to be the United States?” And the question here is ‘is this Italy”? I think it has already proven itself to be in this kind of situation, and what we are trying to do in this country is to make sure that we stay below that capacity of our healthcare system. Because if we have something that looks like this, then this is going to represent the excess deaths, and the reason why this would happen is because of no isolation.
我们在美国这里试图做的是减缓这种情况的发生,以便我们能够照顾到这些进入医院的患者。因此,这里的问题是“这将是美国吗?”这里的问题是“这是意大利”吗?我认为它已经证明自己处于这种情况下,而我们在该国试图做的是确保我们保持在医疗体系的能力之下因为如果我们有一个看起来像这样的东西,那么这将代表过多的死亡,而之所以会发生,是因为没有隔离。
So if you’re wondering why we are doing isolation is that we go on a trajectory of this rather than this. In my clinical practice, and in my administrative practice, in the medical group that I work for, we have spent a lot of time trying to come up with a surge plan and a plan to put into place both in the clinic and in the hospital to actually modify this dotted line for us locally.
如果您想知道为什么我们要进行隔离,是因为我们走的是这个轨迹,而不是这个轨迹。在我的临床实践和行政实践中,在我所工作的医疗团队中,我们花了很多时间来尝试制定一个增值计划,并制定一项既要在诊所又要在医院实施的计划在本地实际为我们修改此虚线。
I like to about that because obviously we’re smart enough to be able to work on two things at the same time: to get this surge down and to flatten the curve. But are there ways that we can raise this bar so that we’re ready to meet this in the middle? So the question is what have we been doing and what are some suggestions that we can give?
我喜欢这一点,因为显然我们很聪明,可以同时处理两件事:降低这种激增并弄平曲线。但是,有什么方法可以提高这个标准,以便我们准备好在中间实现这一目标?因此,问题是我们一直在做什么,我们能提供什么建议?
let’s talk about some of the support that we’re doing. The purpose of this talk is not only to let healthcare providers, clinics, hospitals, out there know what it is that can be done. But it’s also to let all of you know that yes, your healthcare infrastructure is full of people working very hard right now to come up with solutions so that we don’t have to deal with this if we get a surge that we can’t normally deal with.
让我们谈谈我们正在做的一些支持。讲座的目的不仅是让医疗保健提供者,诊所,医院等知道该怎么做。但是,这也要让所有人都知道,是的,您的医疗保健基础设施中挤满了正在努力工作的人们,他们现在想出解决方案,这样,如果我们遇到了无法解决的问题,我们就不必这么处理。
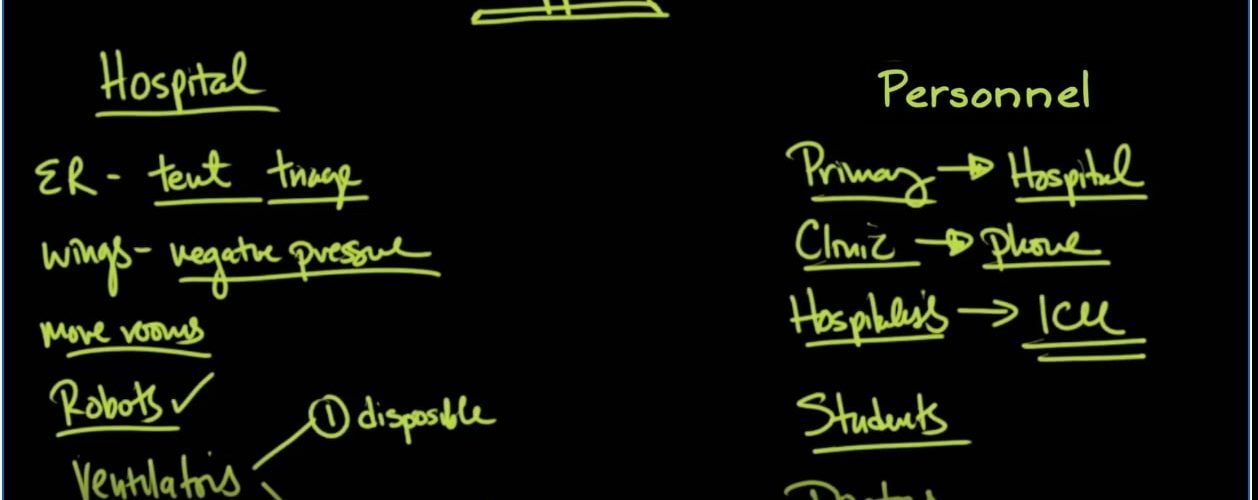
I’m going to divide this into two categories: what we would do at the hospital and what we would do to personnel. These are people and bricks and mortar. The first thing is setting up the emergency room so that there is a pre triage outside, and that usually involves a tent.
我将其分为两类:我们将在医院做的事情和我们将对人员做的事情。这些是人和砖瓦。第一件事是设置急诊室,以便在室外进行预备检查,并且通常涉及一个帐篷。
Sometimes you have to get clearance from your county to be able to treat patients outside of a licensed building. Usually, that can probably happen by this point. If you haven’t already gotten that kind of approval. This tent also allows you to triage people and to put masks on people who may have covid-19 and could spread it to other patients in the emergency room, proper or healthcare providers nurses Etc.
有时,您必须从您所在的县获得许可,才能在许可的建筑物之外治疗患者。通常,这可能会在此时发生。如果您尚未获得这种批准。该帐篷还允许您对人进行分类,并在可能患有covid-19的人身上戴口罩,并可能将其传播给急诊室,适当的或医疗保健提供者等的其他患者。
inside the hospital you can set up whole wings that have negative pressure and we’ve talked about this before the other thing you need to think about is just setting up more rooms these rooms can be other negative pressure Wings whole wings of the hospital, but you have to have engineering look at the situation look at the structure and see how they can configure it so that you’re dealing with a negative pressure room as opposed to a positive pressure room.
You have in the operating rooms.
The other thing that you have to look at is the possibility that some of your providers might be quarantined because they were exposed to somebody with covid-19. And so for that you need to think about robots. So robots are basically computers on mechanical wheels that you can wheel around and they have very powerful microphones speakers and they also have very powerful cameras so that you can see close up and they use these in hospitals where they need in a row.
It’s just 24 hours a day, but they don’t have one. This is the way that they do it for stroke centers, but this could also be very helpful. If you have a physician who’s quarantine at home and can’t come into the hospital but you still need their expertise the last thing that I want to talk about our ventilators so a couple of things on ventilators number one, there are disposable ventilators that you can get fairly cheap and number two is this idea of hooking up multiple patients to ventilators this
It is an off-label use but it’s something that has been done before in an acute surge situation.
So here’s a really cool video that I want you to see and I’m going to put a link to in the description where dr. Babcock and emergency room physician describes in detail how you can take a regular ventilator and actually hook up numerous people to this ventilator and looks as though there are companies that are responding to this video that are actually putting together kits that allow you to readily put ventilators into rooms that allow you to ventilate multiple patients. So I think every hospital in the country should be looking at this.
The as a quick way of temporarily if you need to ventilate patients when you don’t have enough ventilators until you do have enough ventilators.
So let’s talk about Personnel. What do we do? If we don’t have enough doctors primary care doctors typically working in the clinic are seeing well patients. That’s not a priority during a surge. We can take primary care physicians and get them into the hospital many years ago before hospitalist. This is what primary care physicians did they worked in the hospital and in the clinic and even though they might be a little bit Rusty. Some of them are probably well suited to work in the hospital and those
Are the ones that we could select you would have to waive privileges in an acute situation and usually hospital by laws allow for that sort of thing. Especially if it is approved by the chief of staff. What about primary care doctors or clinic patients in general? A lot of those things can be dealt with over the phone. So should you be having elderly patients coming to your office sitting in Waiting rooms? If it is something that can be dealt with over the phone call them up.
And deal with it over the phone. There are some insurance companies that will actually even pay for that kind of a visit if that’s what you’re doing. And obviously they’re going to be visits that you just have to see so these are patients that are being worked up for cancer timely application of tests and reviewing of those tests can be done very quickly. But again, there are still a lot of things that can be done over the phone and if that is the case then that’s what should be done.
What about in the Intensive Care Unit? Well, there are hospitalists people that work in the hospital but not necessarily in the Intensive Care Unit that can help out in the ICU. If it becomes very crowded so hospitalists into the Intensive Care Unit to help out the intensivists who are there. So again, you’re working a little bit out of your area of expertise, but the risks associated with that are far outweighed by the benefits of taking care of people during the surge. What about students?
So this is what happens on a daily basis in teaching hospitals. You have students you have residents. There are able to meet The Surge demand not so much if you have a private hospital where there are no students or residents, but is it possible for students to come into those hospitals to help that has to do with laws that has to do with credentialing and you have to see if those things can be waived to help out in a specific case or cases where you have a surge and you need help what?
Bringing in other doctors, so that’s exactly what’s going on right now here in the United States usually a doctor is licensed to practice medicine in a specific State what has happened is some of those state requirements have been waived. So doctors can travel to other states to help out in Surge situations right now in the United States, not every state is impacted the same as other states are and so it’s possible that doctors from states that are not being impacted could come to those states that are being impacted.
Did so that they can help that’s kind of what’s going on actually right now in Italy but to a much larger extent because you can see the doctors and Italy are having a very difficult time handling this Surge and help is coming from a very unlikely Source. It’s actually coming from China China has had an immense amount of experience in dealing with this coronavirus. You can see here in this article which will put a link to in the description below. So this article goes on to talk about
All of the help and the resources that’s coming from China to help out in Italy which has the most active cases in the world right now the Italian Minister Luigi. Di maio told Rai television. Our doctors don’t need anyone to teach them in their job. But the Chinese doctors were the first to treat the virus and they can bring their experience and this folks is what it’s going to be about when we’re talking about a world pandemic of a deadly virus. We’re going to have to help each other out if we’re going to be able to
to get through this together.
The recipe for Success if we’re going to be able to fight effectively covid-19 is going to come from two different parties. Number one the doctors the nurses the respiratory therapist the hospital’s they are going to have to increase the bar in terms of what we are able to do in terms of our health care abilities, but it’s not just there. Also. We’re going to need help from the public at large to continue ice.
Isolation to make sure that we’re able to flatten that curve. So that’s at the end of the day. We can take care of everybody that we need to take care of. Thanks for joining us.



Add comment