Update 77: Remdesivir Update; COVID-19 in Mexico
本文由‘中国推动’学者、济南大学生命科学学院生物技术专业任紫豪同学编辑整理。
Welcome to another MedCram COVID-19 update and the good news is as you may have noticed is that YouTube has restored all of our videos, so we are full steam ahead.
I wanted to talk a little bit about Mexico. The daily cases in Mexico are increasing steadily, and if we take out the weekend variation, so are the daily deaths. And if we look at the Mexico news daily, we’ll see here that Mexicali overtakes Tijuana to become the number three municipality for COVID-19 cases. Now Mexicali is just across the border from California and the Imperial County of California. And this sudden surge down in Imperial County in the southernmost part of California is overwhelming the medical delivery system down there in Imperial County. And so a number of patients are being moved northward into some parts of LA county and also Riverside County.
Even to the point where nearly 1/3 of patients currently hospitalized for Coronavirus in Riverside County are from neighboring Imperial County. The population of Imperial county is 181000 people which is less than 1/10 of Riverside County’s 2.5 million. And so it looks like there may be a surge of patients in the Southern California area that is related to at least the surge in Mexico.
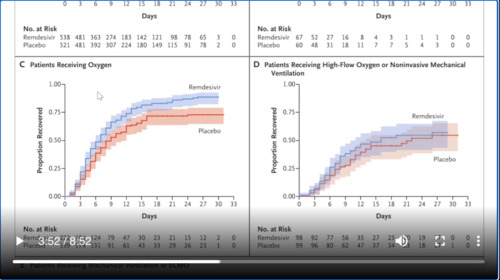
I also wanted to talk a little bit about Remdesivir for the treatment of COVID-19. And this paper was published in the New England Journal of Medicine on May 22nd. What I find really interesting about this study is the difference in the Remdesivir versus Placebo on these kaplan-meier curves. These are survival or recovered curves here and you can see here that blue Remdesivir is higher than Placebo in the overall population. But in B, which is patients not receiving oxygen these would be patients that weren’t sick enough. You can see that there’s quite a bit of overlap between the Remdesivir and the Placebo meaning there was an statistical significant difference.
If we look at C, we can see that patients receiving oxygen or patients sick enough to receive oxygen that there is a difference again between Remdesivir and Placebo. But in D, we have patients here who are receiving a high amount of oxygen or even non invasive mechanical ventilation. That would be like BiPAP or CPAP. These masks that are put on these patients and you can see here that again there is overlap. It needs confidence intervals, meaning that there’s probably not a statistical significant difference.
If we look at patients receiving mechanical ventilation or ECMO, again no difference. Now, this probably makes sense. These people here are too sick and probably have already had the negative effects of the virus. So that killing the virus at this point would be like closing the barn door after the horse has already escaped, whereas in patients here who are not receiving oxygen, these are our patients that aren’t really that sick to begin with and are probably going to do better anyway.
The ones where it really counts would be those that are receiving oxygen but not high flow oxygen or non invasive mechanical ventilation. And again, this is important because I think in a lot of hospitals across the country these hospitals have a very very limited supply of Remdesivir. And so they’re probably going to reserve that very small stash of Remdesivir for the patients that they believe needed the most, the sickest patients. And that very well may be this population and according to this subgroup analysis may not be the ideal population to be getting Remdesivir. The ideal population according to the data are those patients receiving oxygen but not receiving high-flow oxygen or non-invasive mechanical ventilation.
Of course the other reason why is it could be that this population of patients who are receiving oxygen was the largest portion of the patients. And so therefore would have the smallest 95% confidence intervals. They say here the benefit was most apparent in patients with a baseline ordinal score of 5/5 referring to this scale for recovery. They say here a finding most likely due to the larger sample size in this category. So over all these authors conclusions are these preliminary findings support the use of Remdesivir for patients who are hospitalized with COVID-19 and require supplemental oxygen therapy.
However, given high mortality despite the use of Remdesivir, it is clear that treatment with an antiviral drugs alone is not likely to be sufficient. Future strategies should evaluate antiviral agents in combination with other therapeutic approaches or combinations of antiviral agents to continue to improve patient outcomes in COVID-19.
I want to also talk about an interesting article talking about Ford’s police SUVs, which are now being programmed to heat up to 133 degrees to burn the coronavirus away and these will start going out very shortly. So in these vehicles what they’ve done is they’ve programmed the heating system to turn on with the engine and to heat the car up for 15 minutes up to 133 degrees and they find that this is enough to sterilize the interior of the car. They say here in the article that it’s hot enough and long enough to kill more than 99% of disease-causing germs in the vehicle including the coronavirus according to Ford Motor Company.
Once the system is activated, the officer or the technician then leaves the vehicle. The doors are locked automatically as the engine runs at an unusually high idle speed of around 2,000 RPM that heats the engine coolant, which is then used to heat air that’s pumped into the cabin raising the cabin temperature for 15 minutes. And then once the car has been kept hot for 15 minutes or cool down process begins, unheated air outside is pumped into the cabin flushing out the hot air.
And the air condition is switched on after that to cool the cabin down further. So of course, I’m wondering is this going to hurt the interior anyway and apparently it’s well below 176 degrees, which is the temperature that is routinely used in terms of testing. And of course this got me thinking about what I already do when I take my as I call it COVID car to work. This is the car that I’m basically saying. Yes, there could be COVID in my car because it could be on my clothes. But what should I do about it? And this is what I do is I just park it in the sun. And of course it probably gets much hotter in there, especially in these months then 133 degrees and for much longer. And so you can essentially sterilize the interior car by park it in the right place.
I also wanted to highlight this medical news today newsletter titled Science versus COVID-19: Vaccine trial wins and other hopeful findings. And this hope behind the headlines series. They look basically every couple of weeks to see what is the new promising therapeutic approach for COVID-19 and hear the talking about vaccines and COVID-19 convalescent plasma or antibodies from survivors. And so we’ll put a link in the description below but they talk about five things and one of them is that DNA vaccine shows promise in monkeys that there’s a antibody from the a SARS survivor.
That’s the first SARS virus back in 2002. It shows that their antibodies actually can neutralize the current coronavirus that the UK vaccine trial is about ready to enterphase 2 and so there’s some promising news there. And that there is the additional vaccine which appears well tolerated and this was published in the Lancet on May 22nd. And it shows that participants had some mild effects, but for the most part they were short-lived. And that finally convalescent plasma therapy has been deemed to be safe. You know in medicine we say first do no harm.
Now what is convalescent plasma therapy? This is the plasma or the proteins in the blood from patients that have already survived COVID-19 because there’s antibodies in there. They can take those antibodies and put them into patients struggling with the disease currently. And so again, there seems to be some good news here that this is relatively safe.
Thank you for joining us.



Add comment