New Data on Adding Zinc to Hydroxychloroquine + Azithromycin (Lecture 71)
本文由‘中国推动’学者、济南大学生命科学学院生物技术专业任紫豪同学整理。
Welcome to another MedCram COVID-19 update. The number of daily cases in the United States is starting to trend down as are the daily deaths. And that may be because the urban states like New York are starting to see a real reduction in the daily cases and daily deaths in New York. But at the same time in other states were actually seeing an increase or at least a situation where they’re not coming down, like in Texas for instance. Cases in Brazil continue to rise, as are the deaths. It seems as though the daily cases and Russia are starting to plateau, as are the daily deaths in Russia. We’ve also been watching the daily new cases in India.
I want to talk about this article that was submitted from New York University Grossman School of Medicine. Now, this is a preprint. It has not been peer-reviewed but it is a retrospective study looking at hydroxychloroquine, azithromyzin and the addition of zinc in these patients. Now, we’ve talked before about the possible mechanisms of hydroxychloroquine in that it could alter the pH of endosomes and the entrance of the virus into the cell. But there’s some clear data which indicate that hydroxychloroquine and chloroquine may act as a zinc ionophore allowing zinc to come into the cell. And that’s important because zinc inhibits the RNA dependent RNA polymerase or the replicase of the coronavirus.
So the question is whether or not you should give zinc with hydroxychloroquine and this paper sets out to ask whether or not more studies need to be done regarding that issue. So this paper is submitted by Philip M. Carlucci and the paper is titled hydroxychloroquine and azithromycin plus zinc versus hydroxychloroquine and azithromycin alone: outcomes and hospitalized COVID-19 patients. And so the first thing you have to understand is this is a retrospective study. So it’s not going to give us the final say on whether or not hydroxychloroquine and azithromyzin plus zinc is superior. That will only be answered by a prospective randomized controlled trial. Nevertheless, let’s take a look and see what they found.
So interestingly they did note that zinc sulfate may be efficacious against COVID-19 in vitro. And so they started adding it in vivo during the treatment of these COVID-19 patients that were admitted to the hospital. And in fact, these were consecutive patients that were admitted from March 2nd of 2020 through April 5th. And what they found is after adjusting for the time at which zinc sulfate was added to the protocol. They noticed an increase frequency of being discharged home, odds ratio of 1.53 and a reduction in mortality or transfer to hospice remained significant, odds ratio of 0.449. And their conclusion for the study was that this study provides the first in vivo evidence that zinc sulfate in combination with hydroxychloroquine may play a role in therapeutic management for COVID-19. So let’s dig a little deeper.
So in addition to talking about the other modalities that hydroxychloroquine and chloroquine may employ to inhibit the coronavirus, it talks about the fact that zinc inhibits the RNA dependent RNA polymerase. That’s something that we talked about months ago in our COVID-19 updates and has been shown to do this in vitro against SARS-CoV. However, it is difficult to generate, they say, substantial intracellular concentrations of zinc, therefore prophylactic administration of zinc alone may not play a role against SARS-CoV-2. When combined with a zinc ionophore such as chloroquine or hydroxychloroquine, cellular uptake is increased making it more likely to achieve suitably elevated intracellular concentrations. This combination is already being tested as a prophylactic regimen in a randomized clinical trial.
They go on to say that at that New York hospital, they changed some of their practices based on the information that they were getting and so they added zinc sulfate 220 milligrams orally twice daily along with hydroxychloroquine 400 milligrams once followed by 200 milligrams twice daily with azithromycin 500 milligrams once daily to patients at some point along the way. And what they did was they compared retrospectively those patients that got zinc plus hydroxychloroquine and azithromyzin versus those patients that did not get zinc plus hydroxychloroquine and azithromyzin.
So the big thing that you need to do when you look at a retrospective study is look at the two populations and see if one had an advantage over the other and became a confounder. So here we have zinc on the left and no zinc on the right. And we have the P-value and if the P-value is greater than 0.05 then that means that there was no real statistical significant difference. And you can see here that these P-values are for the most point greater than 0.05. When it is less than 0.05, then that means that there is a statistically significant difference between the two. Here we can see. For instance, the respiratory rate had a P-value of 0.046, but you can see here that the range is slightly off and therefore statistically significantly different but not clinically significantly different in this case. Baseline blood pressure also not that clinically significantly different.
Here when we get to the lymphocyte count. We see that the lymphocyte count in the zinc group was higher than the lymphocyte count in the no zinc group. Well, this is statistically significantly different, I’m not sure if 0.1 makes a clinically significant difference. However, having a higher lymphocyte count may give you an advantage and could be used to say that the zinc group did better because of the lymphocyte count rather than the zinc. Similarly, the troponin was higher. The troponin is usually sign of cardiac dysfunction and that was higher in the no zinc group. Now that could be also a cause for why they know zinc group did worse potentially. So these are confounders that you have to take into consideration.
And as you can see here the rest of the medications that were used or not used statistically significantly different in either Group. By the way also mentioned that other medications like Remdesivir or Tocilizumab, the IL-6 inhibitor were not allowed to be included in this study and so patients that receive those medications were not included in this study.
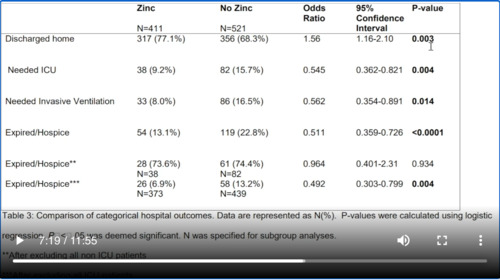
Okay, so let’s talk about these results. Here we have zinc on the left and we have no zinc here on the right. And let’s look at the percentage differences here. So how many patients were discharged home? 77% in the zinc group versus 68.3% in the no zinc group, that was statistically significant. How about those that needed intensive care? 9.2% in the zinc versus 15.7% in the no zinc that was statistically significant. What about needed invasive ventilation? Again, 8% in the zinc group versus 16.5%, again statistically significant. What about expired or had to go to hospice? 13.1% in the zinc group versus 22.8% in the no zinc group that was highly statistically significant.
Now they did something else, if you can see here the two stars that was after excluding all non ICU patient. So these are just the ICU patients. Notice that there really isn’t much difference between these two and notice that we’re no longer statistically significant. And the way that they might interpret that is to say that adding zinc to hydroxychloroquine and azithromycin really helps in those patients who are early in the course and not in the Intensive Care Unit. That once you get into the Intensive Care Unit, you’re now looking to modulate the immune system rather than stop viral reproduction because at that point viral reproduction is no longer the issue but rather inflammation. Here with the three asterisks that is after excluding all ICU patients, so now we’re just looking at the non ICU patients and you can see here clearly that there is a statistically significant difference in the zinc group 6.9% dying versus 13.2% in the no zinc group.
So they recalculate it again and this time they did something called multivariate logistic regression. So in other words, they’re looking at these confounders and seeing if they can eliminate them and see what happened. And so when they did that the things that turn out to be statistically significant is this. Those are discharged home. Notice this time it’s actually lower in the no zinc group. However, when they look at expired versus hospice in the zinc group, it’s lower 13.1% versus 22.8%, higher in the no zinc group and that is statistically significant. So we can definitely see here a mortality difference in this retrospective study, again not totally conclusive. When we look down here, we see another statistically significant situation with all of those where we exclude all ICU patients. So we’re just looking at the non ICU patients here. We can see that the mortality is 6.9% in the zinc group and 13.2% in the no zinc group and again that is statistically significant.
So I think to sum it up the authors themselves say it here. The main finding of this study is that after adjusting for the timing of zinc therapy, we found that the addition of zinc sulfate to hydroxychloroquine and azithromycin was found to associate with a decrease in mortality or transition to hospice among patients who did not require ICU level of care, but that this association was not significant in patients who are treated in the Intensive Care Unit. Further, they say that this result may be reflective of the proposed mechanism of action of zinc sulfate in COVID-19. Zinc has been shown to reduce SARS-CoV RNA dependent RNA polymerase activity in vitro. As such, zinc may have a role in preventing the virus from progressing to severe disease, but once the aberrant production of systemic immune mediators is initiated, known as cytokine storm, the addition of zinc may no longer be effective. Our findings suggest a potential therapeutic synergistic mechanism of zinc sulfate with hydroxychloroquine. If used early on presentation with COVID-19. However, our findings do not suggest a prophylactic benefit of zinc sulfate in the absence of a zinc ionophore, despite interest in this therapy for prevention. A prophylactic strategy of zinc sulfate should be evaluated to help answer this question.
So I thought this study was interesting because it adds credence to many of you who have commented on many of the studies that have been performed in that they did not add zinc to the regimen. And I do think if we are going to answer this question about truly whether hydroxychloroquine works in COVID-19. There’s going to need to be a prospective randomized controlled trial testing hydroxychloroquine and zinc use together. Thanks for joining us.



Add comment