美国睡眠专家详细讲解四类安眠药(苯二氮卓类,非苯二氮卓类镇静剂,褪黑激素激动剂,抗抑郁药)治疗失眠的适用范围、半衰期、副作用等;FDA推荐的使用剂量及特别警告;安眠药的国际前沿研究等。
Video 5 – Insomnia_ Sleeping Pills
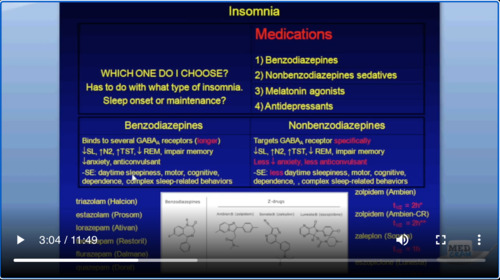
We talked in the last edition of behavioral therapy for insomnia. We went over relaxation technique, sleep restriction therapy, cognitive therapy, and cognitive-behavioral therapy. What we’re gonna talk about next is the part that everybody thinks about when we talk about insomnia. That’s sleeping pills, medications. There are four different classes of medications. They are the benzodiazepines, non benzodiazepines sedatives, melatonin agonists, and finally the antidepressants.
我们在上几段视频讨论了失眠行为疗法。我们讨论了放松技术,睡眠限制疗法,认知疗法和认知行为疗法。接下来我们要谈论的是当我们谈论失眠时每个人都会想到的部分。那是安眠药,药物。有四种不同类别的药物。它们是苯二氮卓类,非苯二氮卓类的镇静剂,褪黑激素激动剂,最后是抗抑郁药。
Medications, in general, do usually improve daytime function. People have better quality of life. There are a few comorbidities, but you’ve got to consider that in general, especially the benzodiazepines, that there are side effects of addiction with time, long-term use. The longer you use a sleeping, the less likely it is to do the job that you intended it to do in the first place. You have more tolerance to these medications.
通常,药物通常可以改善白天的功能。人们的生活质量更高。有一些合并症,但您必须考虑到一般而言,尤其是苯并二氮杂卓类药物,随着时间的推移和长期服用会产生成瘾的副作用。您使用睡眠的时间越长,一开始就无法完成您打算做的工作。您对这些药物的耐受性更高。
What type of patients with these risks goes up? Well, in pregnancy, you have an increased risk of fetal malformations. Also if there’s alcohol consumption going on at the same time, kidney, liver or lung disease certainly. If the patient has sleep apnea, giving them a sleeping pill could make the sleep apnea worse. You really want to be careful in nighttime decision-makers, for example, the people who are on the job, people who are watching alarms, and things of that nature. Finally, the elderly people who are 75 years plus.
哪些类型的患者有这些风险?好吧,在怀孕期间,胎儿畸形的风险增加。另外,如果同时饮酒,肯定会导致肾脏,肝脏或肺部疾病。如果患者患有睡眠呼吸暂停,给他们服用安眠药可能会使睡眠呼吸暂停加重。您真的想在夜间决策者中保持谨慎,例如,正在工作的人员,正在观看警报的人员以及类似性质的事情。最后,是75岁以上的老人。
So this is a busy slide, but let’s go through this methodically. So we’ve got medications. There are four different classes of medications, and let’s talk about the first two classes: benzodiazepines and nonbenzodiazepines. So these nonbenzodiazepines are very similar to benzodiazepines, but they have a different chemical structure.
因此,这是一张繁忙的幻灯片,但让我们有条不紊地进行一下。所以我们有药物。有四种不同的药物类别,让我们谈谈前两类药物:苯并二氮杂卓和非苯并二氮杂卓。因此,这些非苯并二氮杂卓与苯并二氮杂卓非常相似,但是它们具有不同的化学结构。
The benzodiazepines in general, and we’re talking about like triazolam and some of these drugs like Prosom, Antivan, Restoril, Dalmane, and Doral. These all bind to the gaba-a receptors, and there are long-acting. They decrease sleep latency, which is the amount of time it takes to fall asleep. So they do their job. But they also increase that second type of sleep (N2), not REM, not stage 3 sleep, but stage 2 sleep. They also increase total sleep time. So that is intuitive.
一般说来,苯并二氮杂卓类药物和三唑仑类药物以及Prosom,Antivan,Restoril,Dalmane和Doral等其中一些药物在谈论。这些都与gaba-a受体结合,并且具有长效作用。它们减少了睡眠等待时间,这就是入睡所需的时间。因此,他们做了自己的工作。但是它们也会增加第二种睡眠(N2),而不是REM,不是第三阶段的睡眠,而是第二阶段的睡眠。它们还会增加总睡眠时间。这很直观。
They decrease REM; that’s a very interesting characteristic because in patients with REM Behavior Sleep Disorder, where REM sleep seems to be the problem, these benzos actually help. Now, these benzos can cause amnesia, so you have to be aware that they do impair memory. They decrease anxiety. They have also been used as anticonvulsants. As you know, Ativan is a great anticonvulsant.
它们降低了REM;这是一个非常有趣的特征,因为在REM行为睡眠障碍的患者中,REM睡眠似乎是问题所在,这些苯并类化合物实际上会有所帮助。现在,这些苯并可以引起健忘症,因此您必须意识到它们确实会损害记忆力。他们减少焦虑。它们也被用作抗惊厥药。如您所知,Ativan是一种出色的抗惊厥药。
Some of the side effects include daytime sleepiness, motor and cognitive problems with dependence, and complex sleep-related behaviors such as sleep sex, sleep eating, and sleepwalking. There have been many lawsuits associated with people with automatic nocturnal behavior related to benzodiazepines.
一些副作用包括白天嗜睡,依赖的运动和认知问题,以及与睡眠有关的复杂行为,例如睡眠性行为,睡眠饮食和梦游。有许多与苯二氮卓类药物有关的具有夜间活动行为的人的诉讼。
When we look over at the cousins of the benzodiazepines, which are the nonbenzodiazepines, and I’ve got some of their structures down here. So this is the benzodiazepine structure generally speaking, and these are a couple of the other ones. This is zolpidem, which is a nonbenzodiazepine. This is zaleplon, and then finally eszopiclone, which is the same as Lunesta.
当我们查看苯并二氮杂pine的表亲时,它们是非苯并二氮杂s,我在这里有一些结构。因此,一般来讲,这是苯并二氮杂structure结构,它们是另外两个。这是唑吡坦,它是一种非苯并二氮杂pine。这是扎来普仑,最后是eszopiclone,与Lunesta相同。
These three are different in structure to the benzodiazepine. That’s why they’re called the nonbenzodiazepines. But these are probably the ones that you’re familiar with. There are Ambien, Sonata, and Lunesta. So these also target the gaba-A receptors, but they’re born specific; they are cleaner. They do decrease sleep latency. They do increase stage 2 sleep just like their benzodiazepine counterparts; they also increase total sleep time, reduce RAM sleep, and impair memory.
这三个结构与苯二氮卓不同。这就是为什么他们被称为非苯二氮杂类。但是这些可能是您所熟悉的。有Ambien,Sonata和Lunesta。因此,它们也靶向gaba-A受体,但它们天生具有特异性。他们更干净。它们确实减少了睡眠准备期。他们确实像苯二氮卓类药物一样增加了第二阶段的睡眠。它们还会增加总睡眠时间,减少RAM睡眠,并损害记忆。
However, they seem to cause less decrease in anxiety, and they’re less of an anticonvulsant because of their specificity in terms of side effects. We see less of the side effects that we do with the regular benzos such as less daytime sleepiness, fewer problems with the motor, fewer problems with cognitive-behavioral problems, less dependence, and less complex sleep-related behaviors.
然而,由于它们在副作用方面的特异性,它们似乎引起较少的焦虑减轻,并且它们较少作为抗惊厥药。我们看到的与常规苯甲醚相比,副作用更少,例如更少的日间嗜睡,更少的运动问题,更少的认知行为问题,更少的依赖性以及较不复杂的与睡眠相关的行为。
The other important thing is looking at the half-life, which I have listed here. The half-life is important because if you take long-acting sleep medication, and you wake up eight hours later, you could still have this medication hanging around. So it’s important to know the half-life of these medications.
另一个重要的事情是看我在这里列出的半衰期。半衰期很重要,因为如果您服用长效睡眠药物,并且在八个小时后醒来,您仍然可以继续使用这种药物。因此,重要的是要知道这些药物的半衰期。
So Ambient’s got a half-life of two hours, Ambien-CR also two hours. Sonata is pretty short. In fact, it’s the shortest; it’s about one hour. Sonata maybe lasts a little bit longer, and then finally Lunesta is very slow, which is longer-acting and I just think of a slow-moving butterfly if you will. So those are the characteristics of both the benzos and the non-benzos. What I would remember there is that they are both potential causes of dependence, so be aware of that, but the non-benzos are probably cleaner in terms of sleep medication.
Ambien的半衰期为两个小时,Ambien-CR也为两个小时。Sonata很短。实际上,这是最短的。大约一个小时。Sonata的持续时间可能会更长一些,然后最终Lunesta会非常缓慢,这是作用较长的时间,如果您愿意的话,我只是想起一只缓慢移动的蝴蝶。因此,这些都是苯并非苯的特性。我会记住的是,它们都是引起依赖性的潜在原因,因此请注意,但是就睡眠药物而言,非苯并类可能更清洁。
Now recently (this came out in 2013 and you should probably know about this,) the FDA, which has approved the use of Ambien, Ambien CR, Edluar and Zolpimist for sleep, but they were looking at new data, and blood levels in some patients may be high enough the morning after, which could impair activities. So again, they’re sensitive to these long-acting drugs that can cause high levels of sleep medication in the patient’s blood when they’re supposed to be getting up. As a result of that, they recommended lowering the dose specifically in elderly patients.
现在最近(这是在2013年问世的,您可能应该知道这一点),FDA已批准使用Ambien,Ambien CR,Edluar和Zolpimist进行睡眠,但他们正在研究新的数据以及某些患者的血液水平患者可能在第二天早晨足够高,这可能会损害活动。同样,他们对这些长效药物很敏感,这些药物在应该起床时会在患者血液中引起大量的睡眠药物。因此,他们建议降低老年患者的剂量。
Specifically, the FDA warns (in January of 2013) that for Zolpidem: recommended the use of a lower dose in women than previously recommended and also considering this in men as well. Of course, the Ambien CR recommendation was a lower dose and the quote was here that patients should not drive five or engage in other activities that require complete mental alertness the day after taking Zolpidem because Zolpidem levels can remain high enough the next day to impair these activities. So if this is something you want to take on a daily basis, if you read their recommendation, you pretty much shouldn’t be driving. So you’ve got to be aware of these FDA warnings.
FDA特别警告(2013年1月),对于唑吡坦:建议女性使用比先前推荐剂量低的剂量,男性也应考虑使用这种剂量。当然,Ambien CR建议的剂量要低一些,在此引用的意思是患者服用Zolpidem后的第二天不应开车五次或进行其他需要完全精神警觉的活动,因为第二天Zolpidem的水平可能会保持足够高的水平,从而损害这些能力。活动。因此,如果您每天都想这样做,并且阅读了他们的建议,则几乎不应该开车。因此,您必须了解这些FDA警告。
Let’s move on to Melatonin agonists. There’s only one in that category and that’s ramelton, Rozerem. And this is a melatonin agonist, and it binds to M receptors tighter than melatonin does, and it is actually pretty short-acting and because melatonin is used in sleep onset. This medication Rozerem is actually good for sleep-onset insomnia, so if the patient has trouble getting to sleep but has no trouble staying asleep, this might be a good medication for them.
让我们继续研究褪黑激素激动剂。该类别中只有一个,那就是拉梅尔顿,罗泽雷姆(Rozerem)。这是一种褪黑激素激动剂,与褪黑激素相比,与M受体的结合更紧密,而且实际上作用很短,因为褪黑激素帮助进入睡眠。 Rozerem的这种药物实际上对入睡困难型失眠有好处,因此,如果患者难以入睡,但在保持睡眠方面没有任何困难,这对他们来说可能是一个很好的药物。
There are fewer side effects than there are with benzos or nonbenzos, and there are no hypnotic problems symptoms the next day. Now, this is the key point. It’s not habit-forming, so it is not a dependent medication. So if you’re concerned about a patient becoming addicted to sleep medication, this might be the medication for them. It can increase prolactin and decrease testosterone levels; however, the FDA does not at this point see the need to monitor, so this is another medication that may be beneficial.
副作用少于苯并类或非苯并类,并且第二天没有催眠问题症状。现在,这是关键点。它不是养成习惯,因此不是依赖药物。因此,如果您担心患者沉迷于睡眠药物,那么这可能就是他们的药物。它可以增加催乳激素并降低睾丸激素水平;但是,FDA目前没有监测的必要,因此这是另一种可能有益的药物。
Again, antidepressants are the last category. We look at things like doxepine, amitriptyline and trazodone, and this is what I would say if you’ve got a patient who’s depressed and they’re also having problems with sleep, fine, go ahead and pick an antidepressant that also treats insomnia, but I wouldn’t go to an antidepressant as a first-line agent if the patient does not have a psychiatric illness.
同样,抗抑郁药是最后一类。我们会研究多西平,阿米替林和曲唑酮之类的东西,这就是我要说的,如果您患有抑郁症的患者,并且他们的睡眠也有问题,很好,请继续服用抗抑郁药,也可以治疗失眠,但如果患者没有精神病,我不会为患者选择抗抑郁药作为一线药物使用。
So Doxepin is FDA approved, but things like amitriptyline and trazodone are probably not the first-line drugs. I would go to unless the patient also was depressed. So if you look at some of these studies here, “trazodone versus zolpidem,” there was really no difference. So why don’t we go with the one that’s actually FDA approved for insomnia?
因此,多塞平已获得FDA批准,但阿米替林和曲唑酮等可能不是一线药物。我会选择它们除非病人也有抑郁疾病。因此,如果您在此处查看其中的一些研究“曲唑酮与唑吡坦”,实际上没有什么区别。那么,为什么我们不选择经过FDA批准用于失眠的药物呢?
Basically, the sleep societies don’t recommend the use of sedating antidepressants if the patient doesn’t have a psychiatric illness already. So generally speaking, I would stay away from antidepressants unless there’s another reason to choose them.
基本上,如果患者还没有精神病,睡眠协会不建议使用镇静抗抑郁药。因此,总的来说,除非有其他理由选择抗抑郁药,否则我会远离抗抑郁药。
Some of the things that are commonly used are not recommended in terms of the state of the science conference that was done. Benadryl of this is particularly not good in the elderly as it causes a decrease in alertness, cognitive function and increases dry mouth. Antipsychotics: there have only a few trials looking at this and many side effects. Barbiturates: again few trials many side effects.
根据已完成的科学会议的状态,不建议使用某些常用的东西。 Benadryl在老年人中尤其不好,因为它会导致机敏性,认知功能下降和口干增加。抗精神病药:目前只有很少的试验可以观察到这种现象以及许多副作用。巴比妥类药物:再次很少尝试许多副作用。
Some of the things that are done over the counter like valerian, melatonin and alcohol. We’ve already talked about alcohol. It can actually promote sleep disturbance later in the night because of its short-acting nature. Melatonin is not FDA approved. In fact, it’s not even regulated. It’s a nutritional supplement so it can be used in sleep phase delay syndromes, and usually it’s a lower dose that’s going to help, but again reserve my thinking that the medication probably would work better. Valerian does decrease latency by less than a minute. No regulation once again, so you don’t know how much Valerian you’re actually buying when you think you’re buying Valerian, which is not regulated. So again, the sleep societies do not recommend it.
柜台上做的一些事情,如Valeria,Melatonin和酒精。我们已经谈论过酒精。由于它的短效性质,它实际上可以在晚上晚些时候促进睡眠障碍. Melatonin未经FDA批准, 实际上,它甚至没有受到监管。它是一种营养补品,因此可以用于睡眠阶段延迟综合症,通常使用较低剂量的药物会有所帮助,但再次保留我的想法,认为这种药物可能会更好。Valerian确实减少了不到一分钟的等待时间。再次没有监管,因此,当您认为自己购买的未受监管的Valerian,您不知道实际购买了多少Valerian。同样,睡眠协会不建议这样做。
A couple of issues about side effects for older adults. We talked about increasing sleep quality, increase in total sleep time, and decrease frequent awakening. However, there is about a 2-5x time adverse cognitive or psychomotor event. So we got falls; we got fractures, and that goes up.
关于老年人副作用的几个问题。我们讨论了提高睡眠质量,增加总睡眠时间并减少频繁唤醒的问题。但是,大约有2-5倍的时间发生不利的认知或精神运动事件。所以我们跌倒了。我们骨折了,而且上升了。
Interestingly, a study not too long ago showed that mortality went up. This was an observational study rather than a randomized, placebo-controlled trial, so the evidence is not as strong, but it is very concerning that observational studies connected sedative-hypnotics and all-cause mortality to as high as an odds ratio of 4.5. This still needs prospective study data to look at it to see if there’s actually causation as opposed to just association.
有趣的是,不久前的一项研究表明死亡率上升了。这是一项观察性研究,而非随机安慰剂对照试验,因此证据并不充分,但令人关注的是,观察性研究将镇静催眠药和全因死亡率联系在一起,比值比高达4.5。这仍然需要前瞻性研究数据来查看它,以查看是否存在真正的因果关系,而不是仅仅是关联。
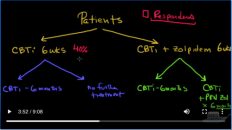
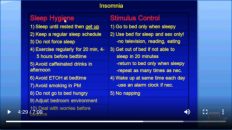
So what do we talked about patients with insomnia? They come into the office. We look for diseases that are easy to rule out. We do hygiene and stimulus therapy and if that still doesn’t work, then we go down the road to behavioral therapy and select medication. Which one do we do first in terms of behavioral therapy and medication? Do we do them at the same time? Do we do one and then the other? What does the data say? Join us for the next lecture where we get into that.
那么关于失眠症患者我们该怎么说呢?他们进了办公室。我们寻找易于排除的疾病。我们进行卫生和刺激疗法,如果仍然无效,那么我们将继续进行行为疗法并选择药物。就行为疗法和药物治疗而言,我们首先要做哪一项?我们是否同时做它们?我们要做一个然后再做另一个吗?数据说什么?和我们一起参加下一个讲座。
Add comment