美国睡眠专家讲解CBTI 及CBTI和安眠药(Zolpidem)混合治疗失眠的效果区别。两组实验分六个星期、六个月和第二个六个月三个周期。结论是效果最好的失眠治疗是CBTI和安眠药(Zolpidem)混合治疗失眠六个星期,之后维持CBTI六个月。
Video 6 – Insomnia_ Putting It All Together
Welcome to another MedCram lecture. In our previous lectures, we talked about insomnia, we talked about what to do in terms of the approach to somebody with insomnia: to look for diseases that we could rule out easily like obstructive sleep apnea; then to do a hygiene questionnaire and a stimulus control questionnaire, or make sure that they were following the recommendations. Then if they still had insomnia after they came back, to establish behavioral therapy and some sort of medication, which we talked about.
欢迎参加另一个MedCram讲座。在以前的讲座中,我们谈到了失眠,我们谈到了针对失眠者的治疗方法:寻找可以轻易排除的疾病,例如阻塞性睡眠呼吸暂停;然后制作卫生调查表和刺激控制调查表,或确保他们遵循建议。然后,如果他们回来后仍然失眠,可以建立行为疗法和某种药物,我们在这里谈到。
But how do we use these together? Do we use one or the other? Do we use both? How long do we use them for? Well, that’s a very good question. Actually, there was a paper that was published in JAMA back in 2009 entitled “cognitive behavioral therapy, singly and combined with medication for persistent insomnia.” So they set out answers to these very questions using a very cleverly designed randomized controlled trial.
但是我们如何一起使用这些?我们使用其中一个?我们两者都使用吗?我们将它们使用多长时间?好吧,这是一个很好的问题。实际上,早在2009年的JAMA上就发表了一篇论文,题为“认知行为疗法,单独并结合药物治疗持续性失眠”。因此,他们使用精心设计的随机对照试验为这些问题设定了答案。
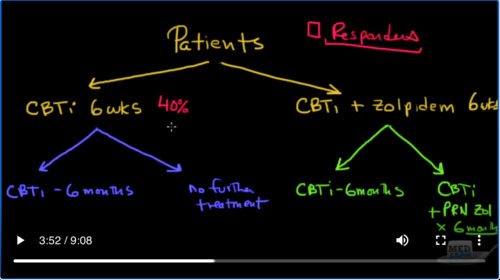
Let’s go over the design of that and see if we can get the answer to really what is the best approach. The first thing they did was they took these patients that were eligible and randomized them into two general groups, which were two treatment groups. One of them was to get CBTI ( or cognitive-behavioral therapy for insomnia) for six weeks. The other would get exactly the same thing: CBTI plus zolpidem, which is a nonbenzodiazepine, also for six weeks.
让我们仔细研究一下它的设计,看看是否可以找到真正最好的方法的答案。他们所做的第一件事是将符合条件的患者分为两组,将其随机分为两个治疗组。其中之一是接受CBTI(或失眠的认知行为疗法)六周。另一个将得到完全相同的结果:CBTI加唑吡坦(一种非苯二氮卓类)也持续了六个星期。
The next thing they did was they would then randomize these two groups into two further groups. After the six weeks of CBTI, one of the groups here would get CBTI for six more months, and the other group would get no further treatment. Now they did the same thing for the other group. They divided this into two further groups. The first group here was divided to get randomization to extended CBTI alone for six months but without the zolpidem; whereas this one was randomized to extended CBTI plus Zolpidem as needed for six months. So this was CBTI + PRN Zolpidem X six months (PRN means as needed).
他们要做的下一件事是,然后将这两个组随机分为另外两个组。经过六周的CBTI治疗后,这里的一组将再接受六个月的CBTI治疗,另一组将不再接受治疗。现在他们为另一小组做同样的事情。他们将其分为两组。第一组分为两组,分别随机接受延长的CBTI治疗六个月,但无唑吡坦。而根据需要将这1个随机分组延长CBTI加Zolpidem,持续6个月。因此,这是六个月的CBTI + PRN唑吡坦(PRN视需要而定)。
So again to review what we have: patients were divided into two groups: cognitive behavioral therapy for six weeks, or cognitive behavioral therapy plus zopidem for six weeks. Then they were further divided, those that only have the CBTI for six weeks were divided for CBTI for another six months, or no further treatment.
因此,再次回顾一下我们所拥有的:将患者分为两组:认知行为治疗6周,或认知行为治疗加唑吡坦6周。然后将它们进一步分割,仅将CBTI维持6周的患者再划分为CBTI,再维持6个月,或者不再进行进一步治疗
To answer the question if the CBTI going on for a long period of time help. The question was is if we give CBTI and Zolpidem together for six weeks, which does better after that? Just CBTI for an additional six months or continuing the Zolpidem for another six months. Now, let me show you the results because the results were actually very interesting.
回答CBTI长期运行是否有帮助。问题是我们是否将CBTI和唑吡坦一起服用6周,那之后效果更好?只需CBTI再维持六个月,或将唑吡坦再维持六个月。现在,让我向您展示结果,因为结果实际上非常有趣。
So let’s look at responders. Basically, what is a responder? A responder is someone who lost their insomnia based on the treatment. So if we look after six weeks of somebody with CBTI, the response rate was about 40%; 40% of the patients responded to the therapy and they got better with just CBTI for six weeks. Now, what was the response rate for CBTI+Zolpidem for six weeks? It was about 45%.
因此,让我们看一下响应者。基本上,什么是响应者?反应者是指因治疗而失眠的人。因此,如果我们照顾一个患有CBTI的人六个星期,其缓解率约为40%。 40%的患者对该疗法有反应,仅使用CBTI治疗6周后病情就好了。现在,六周内CBTI +唑吡坦的缓解率是多少?大约是45%。
So clearly here. The CBTI is the thing that is doing the heavy lifting, with the Zolpidem only having an additional small amount. Now if we look at here at CBTI for six months versus no further treatment, we’re around 45% and around 45%; these are rough numbers. The interesting thing is that if you looked at six-month follow-up after those initial six months, so a year follow-up total, you’re looking at about the same numbers, about 45 percent roughly and 45 percent.
这里很清楚。 CBTI是一项繁重的工作,Zolpidem仅需少量。现在,如果我们在CBTI看六个月而不进行进一步治疗,我们大约是45%和大约45%;这些是粗略的数字。有趣的是,如果您在最初的六个月后进行了六个月的随访,那么一年的随访总数大约是相同的,大约分别为45%和45%。
So this arm clearly shows that you’re not getting many benefits from doing CBTI for six months versus doing just CBTI for six weeks, indicating that CBTI probably has a learning curve that’s pretty quick. However, let’s take a look at this arm over here. So here we have CBTI+Zolpidem, and then we stopped the Zolpidem and just do CBTI for six months, or we continue CBTI with PRN Zolpidem.
因此,这个实验组组清楚地表明,六个月做CBTI比六个星期做CBTI并没有太多好处,这表明CBTI的学习曲线可能很快。但是,让我们来看看这里的这个实验组。因此,这里有CBTI + Zolpidem,然后我们停止了Zolpidem,只做了6个月的CBTI,或者我们继续使用PRN Zolpidem进行CBTI。
So what are the numbers over here? Interestingly, it is around 60 percent. And again, this one is about 60%. What does that mean? That means that CBTI continued after stopping to use Zolpidem was actually better. Let’s compare this number to this number. What’s the only difference? They had CBTI for six months. They had CBTI for six months, but they had it after Zolpidem, but these people did not so, so far this seems to be the best number or even this number seems to be the best number.
那么,这里的数字是多少?有趣的是,它约为60%。再说一次,这一比例约为60%。那是什么意思?这意味着在停止使用唑吡坦后,CBTI仍然更好。让我们将此数字与该数字进行比较。唯一的区别是什么?他们有六个月的CBTI。他们有六个月的CBTI,但他们在Zolpidem之后才得到,但是这些人却没有,到目前为止,这似乎是最好的数字,甚至这个数字似乎也是最好的数字。
But here is the crux of the issue. We did a six-month follow-up on both of these. In other words, CBTI and NO Zolpidem after the initial six-week introduction, and CBTI with PRN Zolpidem to continue. So the question that we’re answering here is yes, we know that CBTI+Zolpidem for six weeks is superior to just CBTI alone. So it’s good to do CBTI or behavioral therapy and add a sleep medication and in this case, is Zolpidem. The question is after six weeks, should we stop it like in this case or should we continue it like we often do in our clinic as the patient needs it?
但这是问题的症结所在。我们对这两方面进行了六个月的随访。换句话说,在最初的六周引入后,CBTI和NO唑吡坦可以继续使用,而CBTI与PRN唑吡坦可以继续使用。因此,我们在这里回答的问题是,我们知道CBTI +唑吡坦治疗6周优于仅使用CBTI。因此,进行CBTI或行为疗法并添加安眠药是一件好事,在这种情况下,它是唑吡坦。问题是六周后,我们应该像这种情况下那样停止它吗?还是应该像患者需要时那样在诊所中继续进行下去?
The six-month (2nd six-month) follow-up was actually very interesting. Actually, have that reversed. The CBTI PRN Zolpidem for six months, dropped to 45 percent. But the 60% of the CBTI only actually increased to 70%. So what all of these results tell us? They tell us CBTI with medication is better than just CBTI alone. Now, it’s not an end statement probably CBTI is more effective than Zolpidem. But together it’s more effective when you do it for six weeks.
六个月(第二个六个月)的随访实际上非常有趣。实际上,已经扭转了这种情况。 CBTI PRN唑吡坦为期六个月,下降至45%。但是CBTI的60%实际上只增加到70%。那么所有这些结果告诉我们什么?他们告诉我们使用药物的CBTI比仅使用CBTI更好。现在,这不是最终结论,CBTI比Zolpidem更有效。但是在一起做六个星期,效果会更好。
The next question is after six weeks, do we continue it on a PRN basis or do we just stop it and do CBTI for the next six months? The answer clearly is that stopping the Zolpidem after six weeks is the best method. As a result of that, the recommendation is combination therapy with CBTI + medications for six-to-eight weeks, then taper the medication and continue the CBTI. So that is the final recommendation.
下一个问题是六周后,我们是否会在PRN基础上继续进行此操作,还是只是在接下来的六个月中停止它并进行CBTI?答案很明显是最好的方法是在六周后停止使用唑吡坦。结果,建议与CBTI +药物联合治疗六到八周,然后逐渐减少药物剂量并继续使用CBTI。所以这是最终建议。
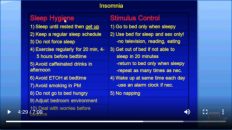
Finally, we can take a look at insomnia and have a general approach here. We talked about how prevalent it is. We talked about some of the reasons why people have insomnia and therefore what our general approaches? Our general approach is to look for diseases initially right off the bat that could cause patients to have insomnia. So things like depression obstructive sleep apnea, restless leg syndrome, these sorts of things. In that absence, then we do sleep hygiene and stimulus control therapy. We see the patient’s back if they still have problems with insomnia, then we engage in behavioral therapy and medication for about 6 weeks.
最后,我们可以看看失眠并在这里有一个一般的方法。我们谈论了它的普遍性。我们谈到了人们失眠的一些原因,因此我们一般会采取什么方法?我们的一般方法是立即寻找可能导致患者失眠的疾病。因此,诸如抑郁阻塞性睡眠呼吸暂停,不安腿综合征等这类事情。在这种情况下,我们需要进行睡眠卫生和刺激控制疗法。如果失眠仍存在问题,我们会看到患者的背部,然后我们进行行为疗法和药物治疗约6周。
We’ve gone over what that behavioral therapy is. Once we’ve done that for six weeks. We continue behavioral therapy for another six months. If that still doesn’t work. Then we can consider sending them to a sleep specialist where other things can be investigated like circadian rhythm disorders and things of that nature again, I would recommend that you do not engage in sleep restriction therapy without supervision. This is serious business. So hopefully this was a good review of insomnia, its approach and the treatment measures. Thank you very much for joining us.
我们已经讨论了行为疗法是什么。一旦我们做了六个星期。我们将继续进行行为治疗六个月。如果那仍然不起作用。然后,我们可以考虑将其发送给睡眠专家,在那里可以对其他事物进行调查,例如昼夜节律紊乱和类似性质的事物,我建议您不要在没有监督的情况下进行睡眠限制治疗。这是严肃的事情。因此希望这是对失眠症,治疗方法和治疗方法的很好的综述。非常感谢您加入我们。

Add comment