美国医学院讲师详细讲解肺部结构及呼吸原理;新冠病毒为什么致命;ARDS(Acute Resporatory Distress Syndrome)造成的肺部损伤;过去二十年抢救ARDS病人的科学进展。
How Coronavirus Kills_ Acute Respiratory Distress Syndrome (ARDS) & Treatment (Coronavirus Lecture 4)
Welcome to another MedCram lecture. So I hear this question a lot. How does the coronavirus actually kill people? There was a recent article in the Lancet that showed that of 41 people that were admitted to the hospital, six of them died, and all of them were on ventilators, and they died with something called ARDS, and ARDS is how the coronavirus kills. It’s not just the coronavirus, but many other viruses including the influenza virus that we have every year.
欢迎参加另一个MedCram讲座。所以我经常听到这个问题。冠状病毒实际上如何杀死人? 《柳叶刀》上有一篇最近的文章显示,入院的41人中有6人死亡,所有人都在呼吸机上死亡,他们死于一种叫做ARDS的东西,而ARDS是冠状病毒的杀死方式。不仅是冠状病毒,还包括我们每年都有的许多其他病毒,包括流感病毒。
How is it that this happens? It’s through acute respiratory distress syndrome, and I’m going to explain to you how that happens. So you first have to understand lung anatomy, and to understand that I like to show you a tree. So a tree has a tree stump, and then it branches, and then those branches branch, and then further those branches branch until finally you get to the leaves. And these leaves capture the sun’s rays, and that’s what gives you photosynthesis, and that’s how the tree lives.
这是怎么回事?这是通过急性呼吸窘迫综合症引起的,我将向您解释这是如何发生的。因此,您首先必须了解肺部解剖结构,并了解我喜欢给您展示一棵树。因此,一棵树有一个树桩,然后它分支,然后是那些分支分支,然后是那些分支分支,直到最终到达叶子。这些叶子捕获了太阳的光线,这就是使您进行光合作用的原因,这就是树的生活方式。
And so what happens is that this tree and the branches increase the surface area of the leaves on the tree so that if you were to pluck off all of the leaves, and you were to put them on the ground next to each other, the surface area that is represented by those leaves would be larger than the shadow that is produced by the sun on that tree.
因此,发生的事情是,这棵树和树枝增加了树上叶子的表面积,因此,如果您要摘下所有叶子,然后将它们彼此相邻地放在地面上,这些叶子代表的区域将大于太阳在那棵树上产生的阴影。
Well, it’s the same exact thing that happens with your lungs. You’ve got an airway, and then that airway divides into a right mainstem bronchus and into a left mainstem bronchus, and then you have a right upper lobe, you have a right middle lobe, right lower lobe, left upper lobe, and you have a left lower lobe. So this is the left side; this is the right, because you’re looking at the patient.
好吧,这与您的肺部发生的完全相同。您有一个气道,然后该气道分为一个右主干支气管和一个左主干支气管,然后您有一个右上叶,一个右中叶,右下叶,左上叶,并且您左下叶所以这是左侧;这是正确的,因为您正在看患者。
And then these things of course divided into much smaller branches, and instead of leaves at the end of all of these things what you have is something called an alveoli, which is a tiny, little, small grape-like structure that the air gets into, and the air of course has oxygen.
然后,这些东西当然会分成许多较小的分支,而不是所有这些东西的末尾都留有叶子,而是所谓的肺泡,它是一种微小的,小的,类似于葡萄的结构,空气进入其中,当然空气中也有氧气。
So what does this look like on a large scale? Here’s what an alveolus looks like. How many alveoli are there in the human body? Well, there’s about 600 million of them. These are very very small. So what happens is deoxygenated blood comes by, and its job is to pick up the oxygen that comes into the alveoli. And then when that oxygen comes in, it oxygenates the blood, and then that blood goes back to the heart, and then to the body, and all your muscles. That’s how you get oxygen. And so you can imagine that this is very very thin because the oxygen which comes down here has to diffuse into the bloodstream.
那么,大范围的情况如何?这就是肺泡的样子。人体中有多少个肺泡?好吧,其中大约有6亿。这些很小。因此,发生的事情是脱氧血液的产生,其工作是吸收进入肺泡的氧气。然后,当氧气进入时,它会为血液充氧,然后血液回到心脏,然后再回到身体,再到所有肌肉。那就是你获取氧气的方式。因此,您可以想象这非常稀薄,因为从这里下来的氧气必须扩散到血液中。
So far so good. But what happens? Well, just like when you hit your finger in the door, your finger swells. That’s because there’s inflammation occurring where you hit your finger in the door, and inflammation causes a leakage of fluids into the tissue space. So what happens here is that you get a viral infection. The virus affects your lungs, and with ARDS the entire lung becomes inflamed, not just in one area like you would have with a pneumonia, or one particular area, for instance, on your finger. And it would just stay in one particular finger, and your whole hand won’t swell.
到目前为止,一切都很好。但是会发生什么呢?好吧,就像当您在门上敲手指时,您的手指会肿胀。那是因为当您在门上敲手指时就会发生炎症,并且炎症会导致液体渗入组织空间。因此,这里发生的是您感染了病毒。该病毒会影响您的肺部,而ARDS会使整个肺部发炎,而不仅仅是像肺炎那样的某个区域发炎,或者手指上的某个特定区域发炎。它只会停留在一根特定的手指上,并且您的整个手不会肿胀。
No. With ARDS, the entire lung goes crazy with inflammation. And so what happens here, instead of having a nice thin area, inflammation goes everywhere, and you get a large barrier a fluid that goes into the interstitial space.
否。使用ARDS,整个肺部会因发炎而发疯。因此,这里发生的是,发炎到处都是,而不是有一个狭窄的区域,而您会遇到一个很大的障碍,即一种液体会进入组织间隙。
Furthermore, these capillaries start to become leaky, and fluid starts to leak into the alveolar space as well. And this starts to fill up with liquid, proteinaceous liquid, liquid that prevents oxygen from getting into the bloodstream. So instead of having nice oxygenated blood, this blood becomes hypoxic, and you become hypoxic if you have ARDS, and you have a hard time breathing, and that’s when you get placed on the ventilator.
此外,这些毛细血管开始渗漏,并且流体也开始渗入肺泡腔。并且这开始充满液体,蛋白质液体,阻止氧气进入血液的液体。因此,这种血液会代替低氧,而不再具有良好的含氧血液,如果您患有ARDS,并且呼吸困难,那就变成了低氧,那就是您被放在呼吸机上的时候。
There’s really nothing you can do to speed this up. There’s nothing that you can do to slow it down. You have to be supported on the ventilator so that you’re getting enough oxygen, and that the machine can breathe for you until, just like everything else after you hit your finger in the door, and the swelling goes away. This fluid will eventually go away as well.
您实际上无法采取任何措施来加快速度。您无法采取任何措施来减慢速度。您必须在呼吸机上得到支撑,以便您获得足够的氧气,并且机器可以为您呼吸,直到您在门上按手指后,其他所有事情都消失了。这种流体最终也将消失。
The key though is keeping you supported during that period of time until the fluid goes away. And then once again, the oxygen will be able to go back into the system, and you will get oxygen back to your tissues.
但是关键是要在这段时间内保持支持,直到油液消失。再一次,氧气将能够返回到系统中,并且您将使氧气回到您的组织中。
So here’s another look at that. We get oxygen that’s going down into these terminal structures called the alveoli. They go into these alveoli, and they cause deoxygenated blood to turn into oxygenated blood, and then go back to the heart.
因此,这是另一种看法。我们得到的氧气会进入这些称为肺泡的末端结构。他们进入这些肺泡,导致脱氧的血液变成含氧的血液,然后回到心脏。
So I’m going to show you three things today that we have learned in the last 20 years that can improve survival in these patients who are on ventilators, to help them beat coronavirus or for that matter any other virus, whether it be influenza, whether it be respiratory syncytial virus, any other kind of virus for beating and getting better if you have ARDS, and you’re on the ventilator.
因此,我今天将向您展示我们在过去20年中学到的三件事,它们可以改善这些使用呼吸机的患者的生存率,帮助他们战胜冠状病毒或就其他任何病毒(无论是流感,无论是呼吸道合胞病毒,还是其他任何类型的病毒,如果您患有ARDS并且正在呼吸机上,都可以跳动并变得更好。
So the first thing that we’re going to look at is what they noticed back in 2000, and actually before, is that when we put people on the ventilator, and the ventilator puts a breath into their airways, what we were trying to do is we’re trying to make sure that we were ventilating patients well.
因此,我们要看的第一件事是他们在2000年之前(实际上是在此之前)注意到的是,当我们将人员放在呼吸机上,并且呼吸机呼气进入呼吸道时,我们正在尝试做的事情我们正在努力确保我们为患者通风良好。
And that’s important in some situations because the blood that is poor in oxygen also has carbon dioxide, which is given up from the muscles. Well, this carbon dioxide would need to be ventilated to be taken out on exhalation, so CO2 will be coming out. Well in order to do that, we have to make sure that enough volume of air was going back and forth, back and forth.
这在某些情况下很重要,因为氧气不足的血液还含有二氧化碳,二氧化碳是从肌肉中释放出来的。那么,这种二氧化碳需要进行通风才能通过呼气排出,因此二氧化碳会散发出去。为了做到这一点,我们必须确保有足够数量的空气来回往返。
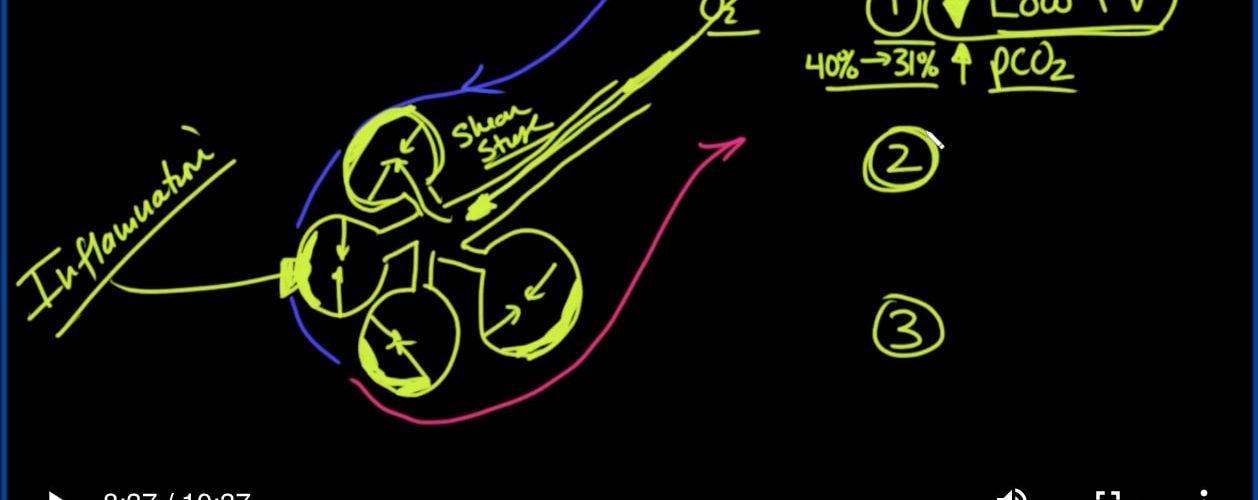
The problem with that though is that we were inflating these alveoli, and then when we were releasing the pressure and letting the air out, these alveoli would collapse down, and nothing was keeping them open. So there would be opening and closing, opening and closing, shutting and opening. And so that was causing a lot of shear stress.
但是,这样做的问题是,我们正在给这些肺泡充气,然后释放压力并释放空气时,这些肺泡会塌陷,没有任何东西使它们保持打开状态。因此将有打开和关闭,打开和关闭,关闭和打开。因此,这引起了很大的剪切应力。
And of course, what’s the whole problem here that we’ve got? Inflammation is what’s causing the whole problem here in the first place, and that’s causing these membranes to become very thick, and the oxygen can’t get in there. And so by ventilating these patients with large tidal volumes, we were causing the inflammation to actually get worse than it would have been if we hadn’t done that.
当然,我们这里遇到的整个问题是什么?首先,炎症是导致整个问题的原因,这导致这些膜变得非常厚,氧气无法进入那里。因此,通过对这些潮气量大的患者进行换气,我们导致的炎症实际上比没有这样做的情况更糟。
And so the scientists started to look at this and say wait a minute. What happens if we just put a lot of pressure down here to keep these alveoli open and only use a small amount of tidal volume to ventilate these patients? And yes, we won’t be able to get as much carbon dioxide out of them, but we don’t really care so long as we’re not adding more inflammation to it. And so the first thing that we looked at this is back in the early 2000s. That this came out is low tidal volume and that would almost certainly cause the PCO2, that is the partial pressure of carbon dioxide in the blood, to go up. So this was called a low tidal volume strategy.
因此,科学家开始研究这个问题,并说请稍等。如果我们在这里施加很大压力以保持这些肺泡开放,并且仅使用少量潮气为这些患者通气,会发生什么情况?是的,我们将无法从其中吸收尽可能多的二氧化碳,但是只要不增加炎症,我们就不在乎。因此,我们研究的第一件事是2000年代初。这是由于潮气量低,几乎可以肯定会导致PCO2(即血液中二氧化碳的分压)上升。因此,这被称为低潮气量策略。
And sure enough, paper was published in 2000 in the New England Journal of Medicine, that showed that we could affect change, and we could decrease the mortality at the time from 40 percent down to about 31 percent mortality. So that was a huge drop in mortality, and all we did was we just ventilated people differently using low tidal volume.
可以肯定的是,论文发表在2000年的《新英格兰医学杂志》上,表明我们可以影响变化,并且可以将当时的死亡率从40%降低到31%左右。因此,这大大降低了死亡率,而我们所做的只是使用低潮气量为人们通风。
Now, when you’re ventilating people with low tidal volume, it’s not very comfortable. They’re trying to breathe more because they don’t like that increased carbon dioxide levels. And so they would try to breathe over the ventilator, and they would try to breathe differently than what the ventilator was telling them to do. And in these cases, we would usually sedate the patients. But if we sedated them too much, bad things could happen to them. They could get blood clots; their blood pressure would go down.
现在,当给低潮气量的人换气时,感觉并不舒服。他们试图呼吸更多,因为他们不喜欢那增加的二氧化碳水平。因此,他们将尝试在呼吸机上呼吸,并且尝试与呼吸机告诉他们的呼吸方式不同。在这种情况下,我们通常会拘束患者。但是,如果我们对它们过度镇静,它们可能会发生不好的事情。他们可能会结块;他们的血压会下降。
And so the second thing that they came up with was actually paralyzing these patients using medications so that they were in perfect sync with the ventilators. And so that was paralysis. Paralysis requires pre-intensive care and intensive care unit. You need good ancillary services, you need respiratory therapist. You need good nursing. Something that you might not get if there’s a huge outbreak, but you could get if attention was made to this.
因此,他们想到的第二件事实际上是使这些患者瘫痪,使他们与呼吸机完全同步。所以那是瘫痪。瘫痪需要重症监护室和重症监护室。您需要良好的辅助服务,需要呼吸治疗师。您需要良好的护理。如果发生大规模爆发,您可能会无法获得某些信息,但是如果对此加以注意,则可能会获得某些信息。
So this paper, also published in the New England Journal of Medicine, (And by the way, I’m going to give links to all of these papers in the description below) they were able to drop the mortality from 41% down to 32%, and this paper was published in 2010.
因此,这篇论文也发表在《新英格兰医学杂志》上(顺便说一下,我将在下面的描述中提供所有这些论文的链接),他们能够将死亡率从41%降至32 %,该论文于2010年发表。
So far so good. What we also started to realize is that patients in the hospital for whatever particular reason. If you ever look at them in bed, they’re always on their back, and what we decided to do was flip them over, and there were a number of reasons for this, so that their belly was down, and that their back was up. We call this prone Positioning.
到目前为止,一切都很好。我们也开始意识到医院的病人出于某种特殊原因。如果您曾经在床上看过他们,他们总是在他们的背上,而我们决定要做的就是将他们翻过来,这有很多原因,他们的腹部向下,而他们的背部起来。我们称之为俯卧位。
And if you do this for about 17 to 18 hours a day, you can actually decrease the mortality, they found, from 33% down to 16%, and this paper was published back in 2013. And so you can see here three breakthroughs in the treatment of ARDS: the final common pathway for morbidity, and mortality in the coronavirus we were talking about.
他们发现,如果每天这样做大约17到18个小时,您实际上可以将死亡率从33%降低到16%,并且该论文于2013年发布。因此,您可以在此处看到三个突破ARDS的治疗:我们正在讨论的冠状病毒发病率和死亡率的最终通用途径。
But the other thing about this, that’s interesting, is we can do a lot if we catch it early, and we get people into the hospital, and we get them in the Intensive Care Unit, and we get them on ventilators, and we’re able to appropriately treat them with good-quality medical care. And three things that really make a difference, then we’ve got a good chance so that they’re not another statistic of mortality, but they survive this.
但与此有关的另一件事是,有趣的是,如果我们及早发现它,我们可以做很多事情,然后将人们送进医院,然后将他们送入重症监护室,然后将他们送上呼吸机,并且能够通过优质的医疗服务适当对待他们。三件事确实有所作为,那么我们就有了很好的机会,使它们不是死亡率的另一种统计数据,但它们可以幸免于难。



Add comment