Aortic Stenosis Explained Clearly
Medcram.com. Hi, welcome to another medcram lecture. We’re going to talk about aortic stenosis and specifically the pathology the pathophysiology and the clinical aspects of this condition. First, I want to just remind you of the anatomy of the heart, for those of you who are starting with this new here,
So we know we’ve got the right atrium.
Which then blood from the right, atrium goes into the tricuspid valve through the tricuspid, valve into the right ventricle. And then that goes out through the pulmonic, valve to the lungs.
from the lungs oxygenated and it goes to left atrium through the mitral valve, then through the aortic valve and then out to the body and then from there
Back to the right atrium. The part that we want to talk about specifically today is the aortic valve, okay? So the aortic valve is the area that we’re talking about and we’re talking specifically about aortic stenosis stenosis simply means closure or the inability for this valve to open. So what are the possible causes of aortic stenosis? Now, we can kind of break this down into those who are 30 years old, or younger greater than 30 years between 30 and 70. And
Greater than 70. So for those who are less than 30 years of age and they get aortic stenosis, that’s pretty rare and the cause of that is calcification of a uni common Cheryl valve. Now what does that mean? The valve usually has three parts. So if you were to look look at it directly on it would look like a Mercedes Benz sign. Well, a unique Amish. Real valve is one that only has one part going through it. Ok, not bicuspid.
But unicorn rasul and these could become calcified. And that’s what we give you. Calcification and stenosis before the age of 30. What’s the most common? Cause between 30 and 70 years of age? That’s bicuspid.
Bicuspid that would be a valve that looks like that. So these become calcified very early and they are the most common cause of aortic stenosis overall and specifically between the ages of 30 and 70. What about, after the age of 70? Here you’ve got a normal valve, you simply get calcification of normal valve, okay? But overall, if they were to ask you what’s the most common cause of aortic stenosis, you would be bicuspid before the age of
70. Okay, so what are we going to see in this type of a situation? Well, because there is stenosis at this area right here, we’re going to start to see that the pressure builds up inside this in this left ventricle. And as a result, the muscle here is going to get thicker than it already is and that’s going to cause what we see in terms of hypertrophy, the compliance of this area is going to go down. And we know that compliance
by definition is the change in volume.
Over the change in pressure. What does that mean? If the compliance goes down then, that means it’s going to take a very large change. In pressure to make a very small change in the volume of this left ventricle. So, what we’re seeing here, in other words, if compliance is going down, is that this is going to become very stiff. Now, why is that important remember
It’s going to be coming in, trying to go into the left ventricle. Now, as a result it’s going to need to fill this up. And if this is very stiff, the pressure in this chamber is going to go up as a result, you’re going to see the pressure in the left atrium also go up. That pressure is going to be transmitted back to the lungs if you’re not careful and as a result that pressure will be transmitted back to the right ventricle.
Cole. So the right atrium and systemically back to the body and you’ll get systemic venous hypertension. Also very briefly as a result of this stenosis here at the aortic valve. There’s going to be less cardiac output and as a result of that, the peripheral vasculature is going to dilate.
This low compliance in the left ventricle is going to make it difficult for these Epi pericardial, blood vessels to supply blood to that area. And as a result, you’re going to actually get a reduction in oxygen perfusion to this muscle over a period of time and that’s even worse than you think. Because it’s going to take more oxygen for this muscle to contract because it has to pump against a higher. What we call after
Good. We’ll talk about after load a little bit in some of the other lectures, but afterload basically is the amount of force or it’s the amount of pressure or tension that this left ventricle needs to overcome and it’s directly related to oxygen consumption. So here you have a situation where oxygen consumption is increasing because of the pressure that needs to be overcome. And yet The myocardium is an in no position to accept the more oxygen because it’s compliance has essentially decreased now as a result of this,
This you get symptoms such as angina or angina, this is pain. Angina pectoris is essentially the same as chest pain. You also get syncope syncope is where you basically pass out. You could also get dis Nia, that’s simply shortness of breath. That’s another symptom of this, a sign is something called pulsus TARDIS.
and also, parviz
This simply means slow and late-breaking, so Tardis is late and parvis is smaller. So the thing is, is that if this valve here, the aortic valve is not opening as well. When the pulse finally gets through and to the peripheral vasculature, when you put your finger on that pulse, it’s going to have a slower up stroke and a later, upstroke, that’s the pulsus parvis, a Tardis. And so some of the complications that you’ll see is something called sudden death
We’re finally become so bad that this valve opens, so little that the heart goes into arrhythmia and you could die. So this is pretty serious. Let’s go over the path of physiology. So as we said, it’s all about the specifics of this valve because this valve doesn’t open. We see a enlargement of the left ventricle and specifically, we see hypertrophy. And so, what we get is after load increasing
So after load goes up and you see thickening of the left ventricular wall, this is called left, ventricular hypertrophy. And this is one of the compensation mechanisms that is used. As we mentioned the wall becomes very stiff. And as a result of that, something called left ventricular, end diastolic pressure and left ventricular, end-diastolic volume increases, but specifically the pressure goes
Up left. Ventricular, end diastolic pressure, simply means what is the pressure in the left ventricle right before it contracts. If that pressure is very high which is what happens in a stiff ventricle. Then the pressure is also going to be high in the left atrium. If that occurs, the left atrial size is going to increase. And the reason is is because the left atrial wall does not have a very thick wall. In fact, it’s very thin, it’s not designed to undergo a lot of
Sure, that can be a problem because if this left atrial wall becomes enlarged, something can happen called atrial fibrillation.
Now, why is that important? If this left ventricle is very stiff, then it’s very difficult for blood to get in to this ventricle for it to be pumped out and you depend very specifically on something called atrial kick. It is the contraction of the Atria right before the ventricle contracts that gets just a little bit more blood back into the left ventricle before gets pumped out through the aortic valve in atrial fibrillation however you
Lose all of that contraction. You see p waves disappear on the EKG. Now there is no more what we call a trail kick. So no atrial kick. And as a result of that, cardiac output drops precipitously. So if you have a patient with aortic stenosis, their left ventricle, starts to increase, then they’re left atrial size starts to increase and that causes atrial fibrillation, they could decompensate very quickly. Now, as we said,
Said because of the increased demand for oxygen and the fact that the compliance of the left ventricular wall is so low. You’re going to get increased oxygen, demand, and decreased oxygen supply. That’s going to cause angina. We already talked about that but and you can also get shortness of breath and you can also get syncope, we talked about that, but the other thing that you’ll see is a low pulse pressure, that means instead of
Something like, 120 over 80 where this is the systolic pressure generated by the force of blood leaving. The left ventricle, and going into the aorta and 80 being a sign of the diastolic pressure. You’ll see that these numbers instead of being 40 apart are going to be much closer to each other because of the stenosis at this aortic valve. And so you might see pressures more along the lines of 110 over. 90, for instance, this is not uncommon to see the
the thing that you will see on your physical examination is that when you examine the patients,
It is normal to listen at the apex of the heart, in this area, which corresponds to this area’s here to find a maximal beat if you will, when you listen, you can also feel this. Now, normally, when the heart gets enlarged, for instance, in congestive heart failure, when the heart becomes enlarged, you’ll see a direction to the left, however, in aortic stenosis because the size of the heart, the size of the left ventricle itself is not increasing, but only the wall thickness. You
See that, the Apex will stay around the same area. The apical impulse, however, will be sustained.
What does that mean? That means that it’s taking a longer period of time to get that blood out through the aortic valve and therefore it will be and hold more time during the time cycle. And so what you see there is you will have a sustained apical impulse which is unmoved. You might also see something called an S for now, if you’ll remember your heart sounds, you remember there is an S 1 and S 1 is simply the sound that is first made in the cardiac cycle.
Swan as you recall is the closure of the atrioventricular valves or the tricuspid valve, and the mitral valve closing, this indicates systole, and goes through until S2 occurs. And if you recall, S2 is the closure of the semilunar valves which are the pulmonic and aortic valves. So, that’s the closure of those. Then you have S3, which apparently is blood coming in and hitting the left ventricle. Usually
It’s a distended left ventricle, that’s why it makes an S3. And so that’s usually indicative of a big distended left ventricle. And then finally S4 which can be heard specifically when the left Atria contract forcing blood into a very stiffened left ventricle. And so what you can see in aortic stenosis is something known as an S4 and that indicates the contraction of this left atrium. Assuming that you’re not an atrial fibrillation, if you are, you will never hear an
For, but if you do get contraction of the left, Atria and S for the blood that goes through hitting a very stiffened left ventricle will cause an S4 and that is a low frequency sound best heard on the left side because the systole begins here between S1 and S2. The type of murmur that you would see is called a crescendo decrescendo and it simply is proportional to the velocity of blood going out of the aorta.
Valve. This is called a crescendo decrescendo murmur and it is heard best at the second right intercostal space. Now as a result of the pathophysiology, anything that increases the gradient around this valve or the amount of blood in the left ventricle is going to increase the murmur, anything that decreases the gradient or decreases, the left ventricular size is going to decrease the murmur. And so what we see here,
That if we decrease, the blood pressure here in the aorta with using things like amyl nitrate.
Abel nightroad will actually decrease the blood pressure in the aorta, which will increase the gradient, and that will increase the murmur of aortic stenosis. If you do something called a valsalva maneuver, which is where you bear down, that usually has the effect of shrinking, both ventricles, both the right and the left as a result of that. Since there’s less blood in the left ventricle to pump through the aortic stenosis doing a valsalva,
will decrease the murmur of aortic stenosis, a few more things in regard to symptoms, specifically, the three symptoms that we talked about known as angina
Syncope.
And congestive heart failure. These three symptoms are very important as a study was done on these and it shows that Angelina is one of the milder symptoms of aortic. Stenosis syncope is a more severe symptoms of aortic stenosis and congestive heart failure is the worst symptom of aortic stenosis and a recent study found that if someone has Angelina
In Arabic stenosis, they have less than five years of life. Expectancy. If someone has syncope, they have less than three years of life expectancy. However, if someone has congestive heart failure, they have less than two years of life expectancy and knowing that order may be testable information. So finally, what’s the treatment?
Well, they do things called balloon valvuloplasty where they actually put a balloon in here and try to open it up, but this is only temporary and it really doesn’t work. The best treatment is actually surgery and there’s two options for surgery, either. You can do something called a bio prosthetic valve.
And by a prosthetic is either made out of pig or cow or bovine Etc. The nice thing about this is that it is not thrombogenic and that you don’t need to be on chronic anticoagulation. So no anti coagulation. The bad thing is however, is that it doesn’t last long.
Doesn’t last 10-plus years so if you have less than 10 years of life expectancy then it’s best to use a bio prosthetic valve. If however you have more than 10 years of life, expectancy than a mechanical valve is the way to go for that. However, you do need anticoagulation.
And the standard of care is warfarin.
With an INR of 2.0 to 3.0 generally speaking. Now the flow past this valve is quite high and so the thrombogenic risk relatively is not as bad as it would be in an area with a slow flow. Now this valve opens, much more and so the flow through here is much slower. As a result, if you had to put a mitral valve replacement in, you would be dealing with an eye on our of 2.5 to 3.5
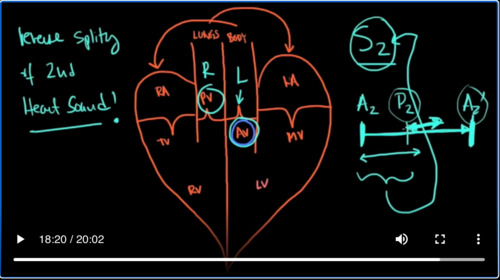
But we’re talking aortic, it’s usually pretty fast. And the recommendation is 2.0 23.0 generally speaking, okay? So that pretty much sums it up. But before I go, I wanted to say one more thing and that’s something that you might see called reverse.
Splitting of second heart sound. So what does this mean? Well, real quick. We’re talking about the second heart sound. As you know, that’s the closure of the aortic valve and the pulmonic valve. Well, in actuality the aortic valve closes first. That’s a 2, and then you get P to, okay? But, it happened so quickly that it’s, we group it into the second heart sound. Well, anything that makes the
Valve or the left side. This is the left side here. This is the right side. Anything that makes the left side delayed in closure of this aortic valve is going to make a 2.
Go in this direction to the point where a to is now after P2. So, how would you know that and why is this called paradoxical? Well, when you take a deep breath in real quickly P2, goes this way. And then, when you breathe out, it comes back this way, this way, for breathing, in this way, for breathing out. And so as a result of that you should see that the difference between a 2 and P 2. In other words, the splitting of that second heart sound should
Get bigger on inspiration and smaller on exhalation. However, if you run into a situation where a to is no longer here and it’s all the way over here. This is still going to move relative to breathing and so when it moves over here, you’re still going to hear this split. But instead of it being larger on inhalation, it’s going to be smaller on him Elation and it’s going to be larger on exhalation. This is exactly the opposite of what you would expect and that’s why it’s called paradoxical or reverse split.
In the second heart sound and it happens because a to gets transposed on the other side of P2. So what would do that? What would cause a to to be so late in relation to P2? Well, it’s anything that causes the left side to slow down relative to the right side or anything that causes the right side to speed up, relative to the left side. So there’s two things that will cause the left side to slow down. One of them is the thing that we’ve been talking about today which is aortic stenosis.
Chaotic stenosis is one of the causes of paradoxical splitting, or reverse splitting of the second heart sound. The other thing is a left bundle branch block. That’s obvious. Why that would slow down. The left side contraction is because there’s a block and the conduction. But the other thing that could cause it is tricuspid regurgitation because tricuspid, regurgitation means, the right ventricle is going to pump blood out of its ventricle faster. Because now it’s got two places to pump it out. And so as a result of that,
The pulmonic valve closes much earlier and P2 goes over here on the other side of a to. And so when it moves, it’s going to cause paradoxical splitting of the second heart sound. I’ll give a lecture on heart sounds and splitting and that sort of thing. But I just want to make sure you knew that aortic stenosis can cause paradoxical splitting of the second heart sound. Thanks very much.

Add comment